Schistosomiasis Control Initiative (SCI) - 2015 Review
We have published a more recent review of this organization. See our most recent report on the SCI Foundation, formerly known as the Schistosomiasis Control Initiative.
More information: What is our evaluation process?
Published: November 2015
Summary
What do they do? SCI works with governments in sub-Saharan Africa to create or scale up programs that treat schistosomiasis and soil-transmitted helminths (STHs) ("deworming"). SCI's role has primarily been to identify country recipients, provide funding to governments for government-implemented programs, provide advisory support, and conduct research on the process and outcomes of the programs. Despite SCI sharing a number of spending reports with us, we do not feel we have a detailed and fully accurate picture of how SCI and the governments it supports have spent funds in the past. (More)
Does it work? We believe that there is relatively strong evidence for the positive impact of deworming. SCI has conducted studies in about half of the countries it works in (including the countries with the largest programs) to determine whether its programs have reached a large proportion of children targeted. These studies have generally found moderately positive results, but have some methodological limitations. (More)
What do you get for your dollar? We estimate that children are dewormed for a total of around $1.26 per child. This figure relies on several difficult-to-estimate inputs including how to account for (a) donated drugs and (b) in-kind contributions from governments with which SCI works. Excluding drugs and government contributions, we estimate that SCI's cost per treatment is $0.53. The number of lives significantly improved is a function of a number of difficult-to-estimate factors, which we discuss in detail in a separate report. (More)
Is there room for more funding? SCI aims to raise a total of $9.5 million for its April 2016 to March 2017 budget year, of which it is on pace to raise $1.7 million absent a GiveWell recommendation and up to $2 million is likely covered by another funder. It aims to raise about $13 million in each of the following two years. If SCI raises more than its goal, it may use funding to treat adults. We have some uncertainty about SCI's room for more funding given past difficulties with predicting how SCI would use additional funds. (More)
SCI is recommended because of its:
- Focus on a program with a strong track record and excellent cost-effectiveness. (More)
- Track record – SCI has repeatedly demonstrated success at starting and expanding national deworming programs.
- Room for more funding – we believe SCI will be able to use additional funds to deliver additional treatments. (More)
Major unresolved issues include:
- We have a limited understanding of SCI's work at a detailed level because we have limited and perhaps unreliable data on how SCI has spent funds in the past.
- The evidence we have seen on SCI's track record of reaching those it has targeted for treatment is fairly limited. We have seen results from about half of the countries SCI has worked in and, for those countries from which we have seen results, we have generally seen one year of results, though SCI has worked in the country for several years. We have some questions about the results we have seen because of methodological limitations of the studies and past challenges communicating with SCI about its monitoring (see blog posts from 2013 and 2014).
Table of Contents
- Summary
- Our review process
- What do they do?
- Does it work?
- What do you get for your dollar?
- Is there room for more funding?
- SCI as an organization
- Sources
Our review process
We began reviewing SCI in 2009. Our review has consisted of:
- Reviewing published studies on SCI's programs.
- Extensive communications with SCI Director Alan Fenwick and Deputy Director Wendy Harrison to discuss SCI's methods and funding needs.
- Requesting and reviewing SCI internal financial, organizational, and monitoring and evaluation documents.
- Visiting a national schistosomiasis control program meeting and demonstration mass drug administration in Malawi in October 2011 (notes and photos from this visit).
- Following SCI's progress and plans for funds raised as a result of GiveWell's recommendation (see our updates on SCI's progress).
- Meetings with eight SCI staff members at SCI's London headquarters in October 2014, including leadership, program managers, and monitoring and evaluation and finance staff.
All content on the Schistosomiasis Control Initiative, including past reviews, updates, blog posts and conversation notes, is available here.
What do they do?
SCI works with governments in sub-Saharan Africa to create or scale up mass drug administration programs (MDAs) for neglected tropical diseases (NTDs), particularly schistosomiasis and soil-transmitted helminths (STHs), in school-aged children and other groups determined to be at high risk.1 SCI's role has primarily been to solicit grants from large funders, identify country recipients, provide funding to governments for government-implemented programs, provide advisory support, and conduct research on the process and outcomes of the programs.
We feel that we have a limited understanding of SCI's work at a detailed level. SCI's model involves both (a) employing staff for program management and technical assistance (capacity building) and (b) funding governments to carry out mapping and treatment programs. We have a reasonable understanding of the role SCI's staff plays, but have struggled to get a clear and complete picture of how SCI and the governments it supports have spent funds in the past. Clear spending data would allow us to have a better understanding of SCI's model, have more confidence in its financial management (including whether funds may be diverted for uses that don't support the program), and compare future plans to past spending to understand whether future funds are likely to achieve similar outcomes.
Major funding sources for SCI's work
Large grants
SCI's work has been driven by a number of large grants, each with somewhat different program designs and geographic coverage. SCI's major grants:
- Initial Gates Foundation grant: SCI was founded in 2002 through a $32 million grant from the Bill and Melinda Gates Foundation.2 This grant was used to create national treatment programs for schistosomiasis and soil-transmitted helminths (STHs) in six countries.3
- Grants for integrated NTD control: In 2006, SCI received large grants from USAID and the Gates Foundation to support integrated NTD programs in eight countries for five years to treat lymphatic filariasis, onchocerciasis, and trachoma, in addition to schistosomiasis and STHs.4 It received a grant in 2007 to expand its work to Rwanda and Burundi.5 All of these grants were completed in 2011.6
- DFID grants: In 2010, SCI received £10.5 million7 (plus separate funding for drugs) from the UK's Department for International Development (DFID) for treating schistosomiasis and soil-transmitted helminths8 in eight countries over five years.9 Other NTDs are not covered by the grant, though DFID also provided funding to the Filarial Programmes Support Unit (FPSU; formerly the Centre for Neglected Tropical Diseases) to integrate treatment for lymphatic filariasis with SCI-funded schistosomiasis and STH programs in six countries.10 In 2014, DFID awarded SCI an additional £16.6 million over four and a half years (June 2014 to December 2018) to extend the program and expand it to an additional two countries.11
Unrestricted funding
Prior to 2011, unrestricted funds accounted for a very small portion of SCI's total funding.12 SCI told us that this funding was primarily used to fund treatments in regions of Côte d'Ivoire and Mozambique.13
In part due to GiveWell's recommendation, since November 2011, SCI has received significantly more unrestricted funds: GiveWell has tracked about $11.4 million in donations to SCI due to our research.14 We estimate that at least 70% of the unrestricted funds that SCI raised in April 2013 to March 2015 (the period for which we've seen data) were due to GiveWell's recommendation.15
Unrestricted funds now make up a large portion of SCI's revenue. For April 2013 to March 2015, SCI reports that 61% of its revenue was unrestricted (though we believe that some non-DFID restricted funds are classified as unrestricted in this report, see below).16
SCI’s role in mass drug administration programs
SCI's role in mass drug administrations (MDAs) in general is to:17
- Advocate for the benefits of mass drug distributions to government officials.
- Assist with planning and budgeting.
- Deliver funding and drugs to governments.
- Provide financial management and technical support.
- Develop procedures for monitoring and evaluation, analyze data, and write reports.
In 2014, we spoke with four of SCI's program managers to better understand SCI's role in four countries. These conversations were mostly consistent with our general understanding of SCI's work. We selected Côte d'Ivoire, Ethiopia, and Mozambique because SCI has spent significant unrestricted funds, the type of funding GiveWell has recommended, in these countries. SCI selected Uganda as the fourth case study. Summaries follow.
In addition, in 2015, SCI shared some details about its work in Sudan, where it recently began supporting a program, and in Nigeria, where it is considering supporting a program in the future. We have not yet written up summaries of this work (documents SCI shared listed in footnote).18
Côte d'Ivoire
- History: There was no large-scale schistosomiasis treatment program in the country prior to SCI's involvement.19 SCI began working in Côte d'Ivoire in 2010, but mapping and treatments did not begin until 2012 due to political turmoil. It has funded mapping and treatment for all qualifying districts.20 SCI expected to fund about 4.9 million treatments during its 2014-15 budget year;21 it reported delivering 3.1 million treatments in that period.22 SCI previously told us that it spent a small amount of unrestricted funding in the country prior to 2011; we do not know what this funding was for.23
- Current plans (as of October 2015): SCI plans to deliver 0.4 million treatments in its 2015-16 budget year, 2.7 million treatments in its 2016-17 budget year, and 2.3 million treatments in each of the following two years. These plans may be dependent on SCI's fundraising.24
- Funding: SCI has used DFID funding, a grant from the company Vitol, and unrestricted funding in Côte d'Ivoire.25 In the 2014-15 budget year, SCI spent about $250,000 in restricted funding and $820,000 in unrestricted funding in the country, a significant increase over 2013-14, when SCI spent $580,000 in restricted funding and $20,000 in unrestricted funding.26
- Impact of unrestricted funds: SCI believes that availability of unrestricted funds has allowed the program to scale up faster than it otherwise could have.27
- Partners: In the early stages of the program, SCI primarily worked with the Ministry of Health and, for mapping, the Université Félix Houphouët-Boigny. Starting in 2014, SCI began working with other partners, including Sightsavers, the END Fund, and Helen Keller International on a more integrated NTD program.28
- Role of SCI staff: SCI's Program Manager for Côte d'Ivoire described her role (as of October 2014) as providing technical expertise, helping create budgets, monitoring training and MDAs, responding to problems (for example, surveying health workers to understand low coverage of non-enrolled children, and advising on how to proceed with the program during a security threat), refining the protocol for the coverage survey, and coordinating with partners for integrated MDAs.29 From November 2013 through November 2014, she traveled to Côte d'Ivoire five times and spent almost four months there in total to assist with and monitor mapping, sentinel site and coverage survey data collection, three MDAs, and budgeting.30 She also noted the role of other SCI staff in the program: the finance team checks receipts against expense reports,31 and the biostatistician analyzes monitoring data and advises government staff on data issues.32
Ethiopia
- History: There was no sustained, large-scale schistosomiasis treatment program in the country prior to SCI's involvement, only a one-off, sub-national treatment.33 SCI began conversations with the government of Ethiopia about starting a national schistosomiasis treatment program in 2012. In 2013, it funded planning for the program. It funded mapping between November 2013 and April 2014, and a first round of treatment in 2013.34 In April 2015, Ethiopia treated a reported 2.9 million children for schistosomiasis and STH. SCI planned to conduct a coverage survey following this round of treatment and collected baseline data on infection rates from 22 sentinel schools prior to the treatment round (more on these data collection methods below).35 We have not yet seen results.
- Current plans (as of October 2015): SCI reports that it had delivered 2.9 million treatments between April and September 201536 and plans to deliver a total of 10.6 million treatments in its 2015-16 budget year. It also plans to deliver 14.4 million treatments in its 2016-17 budget year and about 17 million treatments in each of the following two years. These plans may be dependent on SCI's fundraising.37
- Funding: SCI used about $1.7 million in unrestricted funds for planning, mapping, and the first two rounds of treatment.38 The END Fund and DFID have now allocated restricted funds for treatment in the country.39
- Impact of unrestricted funds: SCI believes that availability of mapping data significantly improved the chances of securing funding from the END Fund and DFID, and that, at a minimum, the availability of unrestricted funds accelerated the program by a few years.40 Ethiopia's Neglected Tropical Diseases Program Manager told us that the government had not dedicated funding to schistosomiasis and that without SCI's involvement the program would likely not have gone forward. According to him, Ethiopia was not aware of any other potential partners for this work when it began working with SCI.41
- Partners: SCI is funding the Federal Ministry of Health (FMOH) to carry out treatments. It partnered with the Ethiopian Public Health Institute, the technical arm of the FMOH, and the Partnership for Child Development (PCD) on mapping. PCD funded mapping in part of the country and delivered treatments in a pilot program. Deworm the World Initiative is providing technical assistance to the government.42
- Role of SCI staff: SCI's Program Manager for Ethiopia described his role (as of October 2014) as assisting with initial program set up and funder agreements, drafting detailed plans for the next 12 months and general plans for the next 5 years, and providing technical assistance for mapping and some guidance on MDA implementation. He lives in the country43 and works in the same office as the government NTD team.44
Mozambique
- History: There was no large-scale schistosomiasis treatment program in the country prior to SCI/FPSU's involvement. SCI had previously funded a small-scale treatment program in Mozambique with unrestricted funding.45 SCI's grant from DFID, which started in 2010, includes funding for a sub-grant to FPSU to run schistosomiasis treatment programs in three countries, one of which is Mozambique.46 SCI and FPSU decided on this arrangement because SCI believed it would increase the chances of DFID awarding the grant.47 SCI reports that it delivered 14.3 million treatments between April 2011 and March 2015.
- Current plans (as of October 2015): SCI reports that it had delivered 4.4 million treatments between April and September 201548 and plans to deliver a total of 5.4 million treatments in its 2015-16 budget year. It also plans to deliver 9.6 million treatments in its 2016-17 budget year and 16.8 million treatments in each of the following two years. These plans may be dependent on SCI's fundraising.49
- Funding: SCI has spent both restricted funding from DFID and unrestricted funding in Mozambique. The data we have seen on SCI's spending in Mozambique is incomplete (see below), but our impression is that Mozambique has been one of SCI's largest programs.50 It has funding from the SCORE project for research on "gaining and sustaining control of schistosomiasis" in one province.51
- Impact of unrestricted funds: SCI told us that unrestricted funds have helped the program scale, but perhaps not as much as it might appear, since SCI has shifted DFID funding to other countries with the expectation of using unrestricted funds in Mozamique.52
- Partners: The Ministry of Health implements the program. SCI/FPSU also collaborate with RTI International, which is working on trachoma in Mozambique and has staff in-country. RTI helps to keep SCI/FPSU informed about program progress.53
- Role of SCI staff: FPSU manages the program day-to-day. SCI has provided some assistance with monitoring and evaluation. We do not have more detail on SCI/FPSU role in the country.54
Uganda
- History: SCI has worked in Uganda since 2003 and has received funding for this work from each of its large grants: Gates Foundation, USAID, and DFID. There was a gap in SCI's work between the USAID and DFID funding.55 SCI reported that it delivered 23,000 treatments in April 2014 to March 2015.56 It had planned to fund 400,000 treatments this period;57 we haven't discussed with SCI why significantly fewer treatments were delivered than planned.
- Current plans (as of October 2015): SCI plans to deliver 1 million treatments in its 2015-16 budget year, 1.8 million treatments in its 2016-17 budget year, 1.4 million in 2017-18 and 1.8 million in 2018-19. These plans may be dependent on SCI's fundraising.58
- Funding: In recent years, SCI has primarily used DFID funding in Uganda (about $176,000 in the fiscal year covering 2013-14 and $30,000 in 2014-15).59 SCI allocated a small amount of unrestricted funding to Uganda to increase the number of sentinel sites for operational research purposes.60 SCI also spent about $30,000 in unrestricted funds in Uganda in 2014-15;61 we don't know what these funds were used for.
- Partners: RTI International, funded by USAID, works in Uganda on an integrated mass NTD treatment program. SCI provides schistosomiasis treatment in those areas where RTI does not.62
- Role of SCI staff: SCI told us that, due to strong in-country capacity, SCI provides only limited technical assistance for MDA. Instead, SCI's technical assistance in the country is focused on operational research on how best to move toward elimination of schistosomiasis.63 SCI's program manager for Uganda describes her role as (as of October 2014) assisting with budgets and plans, talking to the government regularly (largely through email) leading up to an MDA to make sure all the components are prepared, traveling to the country to oversee collection of prevalence and intensity data prior to an MDA, following up with the government after an MDA to get the data needed for reporting to DFID, and participating in activity reviews after each stage of the program (for example, after an MDA and after monitoring and evaluation activities).64
Breakdown of SCI’s spending
We have seen fairly limited information on how SCI has spent funds in the past. SCI has only recently compiled a comprehensive report of all of its expenditures. We know of several limitations to this report and are not confident that the report is complete and fully accurate.
Limitations to the spending information we've seen
There are several structural reasons to be cautious about interpreting the data:
- SCI is housed within Imperial College London. Because it is not a standalone charity, it does not publish annual financial statements or undergo annual organization-wide audits (as U.S. charities are required to do).
- It uses an accounting system created by Imperial College which seems ill-fitted to its needs and which breaks up its finances into many different "accounts" rather than giving an overall view of the organization's financial position.65
- SCI has noted that its financial systems need improvement and has been working to expand its accounting team and improve its systems.66 SCI's current Finance and Operations Manager joined the organization in mid-2015 after the previous Finance and Operations Manager left the organization after about six months.67
- Based on our experiences with SCI's financial reports, we believe that they are prone to containing errors. We detail the errors we have learned about in this footnote.68
In addition, the information we have seen is limited in scope:
- We have only seen comprehensive data for two budget years: April 2013-March 2014 ("2013/14") and April 2014-March 2015 ("2014/15").
- We have not seen recent information on how much funding SCI currently holds or on what portion of the funds that it holds are committed and uncommitted.
- We have not seen complete or recent information on how SCI has spent funds within country programs. The data we have seen is only broken down by country.
- The data we have seen only tracks funds to the point of being transferred to accounts within the countries that SCI works in. Therefore, some of the recorded expenditures do not represent actual spending. We don't know how long funds typically sit in in-country accounts before being spent.
Spending breakdown
Notes about this data:
- For Zambia, Liberia, and Mozambique, SCI transfers funds to FPSU, rather than directly to the country. SCI told us that it has not yet been able to break out some of that funding and so some of those payments are included in "central programme expenditure" rather than the total for the country program, particularly in the 2013/14 data. SCI believes this is the main reason why it appears that central expenditure falls significantly in 2014/15.69
- Some restricted grants other than funds from DFID (such as funds from the END Fund or large donors who have restricted their funds to a specific country) are included in the unrestricted revenue total, while the expenditures from these grants may be included in the totals for restricted expenditure.70 We do not know how much funding these grants account for.
For full details see SCI financial statement 2013/14 and 2014/15 (revised October 2015).
2013/14 expenditures by country (in millions USD)
| Restricted | Unrestricted | Total | % of total | |
|---|---|---|---|---|
| Central expenditure | $1.27 | $0.65 | $1.92 | 28.5% |
| Ethiopia | - | $1.15 | $1.15 | 17.1% |
| Burundi | $0.49 | $0.20 | $0.69 | 10.3% |
| Tanzania | $0.65 | - | $0.65 | 9.7% |
| Côte d'Ivoire | $0.58 | $0.02 | $0.60 | 8.9% |
| Uganda | $0.28 | $0.10 | $0.38 | 5.6% |
| Malawi | $0.27 | $0.10 | $0.37 | 5.5% |
| Niger | $0.30 | - | $0.30 | 4.5% |
| Zanzibar | $0.27 | $0.01 | $0.28 | 4.2% |
| Yemen | $0.13 | - | $0.13 | 1.9% |
| Rwanda | $0.08 | - | $0.08 | 1.2% |
| Zimbabwe | - | $0.07 | $0.07 | 1.0% |
| Mauritania | - | $0.06 | $0.06 | 0.9% |
| Mozambique | $0.05 | - | $0.05 | 0.7% |
| Total | $4.37 | $2.36 | $6.73 | 100.0% |
2014/15 expenditures by country (in millions USD)
| Restricted | Unrestricted | Total | % of total | |
|---|---|---|---|---|
| Central expenditure | $0.78 | $0.28 | $1.06 | 15.1% |
| Mozambique | $0.22 | $1.03 | $1.25 | 17.8% |
| Ethiopia | $0.64 | $0.58 | $1.22 | 17.3% |
| Côte d'Ivoire | $0.25 | $0.82 | $1.07 | 15.2% |
| Malawi | $0.52 | - | $0.52 | 7.4% |
| Sudan | - | $0.37 | $0.37 | 5.3% |
| Rwanda | $0.34 | - | $0.34 | 4.8% |
| Democratic Republic of the Congo | $0.34 | - | $0.34 | 4.8% |
| Zanzibar | $0.19 | $0.06 | $0.25 | 3.6% |
| Burundi | $0.15 | $0.05 | $0.20 | 2.8% |
| Yemen | $0.12 | $0.01 | $0.13 | 1.8% |
| Uganda | $0.05 | $0.05 | $0.10 | 1.4% |
| Madagascar | $0.09 | - | $0.09 | 1.3% |
| Liberia | - | $0.07 | $0.07 | 1.0% |
| Tanzania | - | $0.02 | $0.02 | 0.3% |
| Niger | $0.01 | - | $0.01 | 0.1% |
| Total | $3.70 | $3.34 | $7.04 | 100.0% |
DFID grant spending breakdown
We have not seen comprehensive data on how funds have been spent within country programs, but we have seen some data from seven countries: Niger, Tanzania, Uganda, Malawi, Mozambique, Zambia, and Liberia over two to three years, mid-2011 to 2013 or 2014 (actual periods vary by country).71 SCI told us that these are the only countries for which it has completed this type of spending analysis.72 We do not know why these particular countries were selected, but note that they are countries that are either funded by DFID and have received little or no unrestricted funds73 or country programs that are managed by FPSU.74 SCI has a long history of involvement in Niger, Tanzania, and Uganda, so we would guess that these programs are at a more advanced stage of development than many of the countries where SCI has begun working more recently.
In-country SCI spending in seven countries75
| Budget item | % of spending | Description | Range across countries |
|---|---|---|---|
| Mass drug administration | 40% | Largely unspecified transfers to districts, individuals, or other organizations; per diem payments for health workers and supervisors; production of dose poles and treatment registers. | 9% to 76% |
| Mapping (surveys to determine disease prevalence in each district) | 19% | Per diem payments; fuel and transport; equipment; utilities | 0% to 50% |
| Monitoring and evaluation (baseline and follow up surveys of prevalence and intensity; coverage surveys) | 9% | Per diem payments for attendance at review meeting; per diem payments for surveyors; fuel and transport; equipment | 1% to 22% |
| Training | 8% | Limited details | 0% to 29% |
| Central management (country-level) | 8% | Salaries for government staff; fuel and transport; utilities; office supplies and equipment; taxes; bank charges | 0% to 47% |
| Advocacy and social mobilization (building community awareness of the program) | 8% | Printing; radio and TV broadcasts; unspecified per diem payments | 1% to 30% |
| Supervision | 3% | Per diem payments; fuel and transport | 0% to 7% |
| Strategic planning | 2% | Per diem payments; meeting venue and refreshments; fuel and transport; supplies | 0% to 8% |
| Drug supply chain | 2% | Custom fees; transport; per diem payments; lab materials; storage | 0% to 4% |
Other projects
In addition, SCI has received some smaller grants for a variety of projects, including:
- Research. SCI has received a number of smaller grants to carry out research related to NTD control.76
- Other NTD-related activities. SCI has also used funding from individuals for surgeries for hydrocele (a symptom of lymphatic filariasis) in Niger, and health education and water and sanitation programs in Burundi.77
Does it work?
SCI's mass drug administration programs are focused on delivering treatments that have been independently studied in rigorous trials and found to be effective.
SCI has conducted studies in some of the countries it has worked in to determine whether its programs have reached a large proportion of children targeted. We have now seen some recent monitoring results from about half of the countries in which SCI works, including the five countries where SCI has delivered the largest number of treatments. For those countries from which we have seen monitoring results, we have generally seen one year of results, though SCI has worked in the country for several years. We have some questions about the results we have seen because of methodological limitations of the studies.
To determine SCI's track record at executing programs, we have considered:
- Studies of changes in prevalence and intensity of infection over time in three of the countries SCI has worked in. The studies show substantial improvements following SCI treatment programs. These studies have a number of limitations and represent a small portion of SCI's past work.
- Treatment coverage surveys from six of the countries SCI has worked in, including many of the countries where SCI's work has been focused in the past five years. These studies track what percentage of individuals who were targeted for treatment actually received treatment. Overall, the studies found moderate rates of coverage. We note some limitations of these studies below.
- Other published papers that might reflect the treatment coverage achieved by SCI's programs by directly measuring deworming drug uptake or by measuring worm prevalence in countries where SCI has worked. The evidence is mixed, but makes a weak case for low coverage in the areas studied.
Details follow.
Independent evidence of program effectiveness
SCI's primary program is mass combination deworming, which we discuss extensively on another page. There is a very strong case that mass deworming is effective in reducing infections. The evidence on the connection to positive quality-of-life impacts is less clear, but there is a fairly strong possibility that deworming is highly beneficial.
Prevalence and intensity studies
SCI has conducted studies to track changes in schistosomiasis and STH prevalence and intensity rates following SCI-supported treatment programs. In each of these studies, SCI tracked infection rates at the same schools ("sentinel sites") each year. In general, prevalence and intensity of the parasites decreased over time in each of the countries studied. We note several methodological limitations of these studies below.
Which prevalence and intensity studies provide evidence of SCI's impact?
Below, we discuss results from studies of schistosomiasis and STH prevalence and intensity from three countries: Niger (2004-2006),78 Burundi (2007-2010),79 and Malawi (2012-2015).80
SCI also shared studies from Uganda81 and Burkina Faso,82 and we included results from these studies in our previous reviews of SCI. We learned in 2013 (and in follow up work in 2014) that participants in the studies in Uganda and Burkina Faso received separate, more intensive treatment than other children in those countries (discussed in blog posts in 2013 and 2014). Therefore, we believe that the results from Uganda and Burkina Faso do not reflect the quality of the national programs which were supported by SCI.
It is our understanding that, in the Niger, Burundi, and Malawi studies, study participants received treatment in the same manner as other children in the country, and thus that those studies reflect the performance of the national MDAs. However, we are not highly confident in this conclusion because we had difficulties communicating clearly with SCI about the methodology of these studies (discussed in more detail in the blog posts linked above).
SCI told us that it is currently conducting similar studies in Mozambique, Ethiopia, DRC, Liberia, Côte d'Ivoire, Zambia, Tanzania, Uganda, and Niger (for more recent years). We have not yet seen results from any of these studies.83
Niger, Burundi, and Malawi prevalence and intensity studies
As discussed above, SCI has conducted studies to track changes in schistosomiasis and STH prevalence and intensity rates following SCI-supported treatment programs in Niger, Burundi, and Malawi. In each study, with one exception, the same individuals were examined before the initial round of treatment and before each subsequent round of treatment.84 In the 2015 Malawi study, SCI switched to a cross-sectional sample, where random children from the same schools were surveyed, rather than the same individuals.85 To partially account for this change, the data from Malawi presented below is for the 6-8 year old age group only. There is no control group for these studies.86
In general, prevalence and intensity for the two main types of schistosomiasis, S. haemotobium and S. mansoni, and for hookworm (more on the other two STHs below), decreased over time in each of the countries studied. Though it is possible that other factors besides the treatment program caused these changes (such as improved sanitation infrastructure), the pattern of decline in a short period following treatment strongly suggests that treatment caused or contributed to the declines.
Changes in worm prevalence and intensity87
| Schistosoma haematobium | Schistosoma mansoni | Hookworm | ||||
|---|---|---|---|---|---|---|
| Country | Changes in prevalence | Changes in intensity | Changes in prevalence | Changes in intensity | Changes in prevalence | Changes in intensity |
| Niger | 75.4% at baseline to 38% at one year88 | 21.8% prevalence of heavy-intensity infections at baseline to 4.6% at one year89 | Very low prevalence at baseline90 | N/A | Low prevalence at baseline91 | N/A |
| Burundi (pilot) | Not reported (SCI reports very low baseline prevalence92 ) | N/A | 12.7% at baseline to 1.7% at four years93 | 20 epg94 at baseline to 1 epg at three years95 | 17.8% at baseline to 2.7% at four years96 | 16 epg at baseline to 24 epg at three years97 |
| Burundi (other schools) | Not reported (SCI reports very low baseline prevalence98 ) | N/A | 6.2% at baseline to 0.7% at three years99 | 15 epg at baseline to 8 epg at one year100 | 15.1% at baseline to 5.4% at three years101 | 15 epg at baseline to 8 epg at one year102 |
| Malawi | 9% at baseline, 6% at one year, 4% at two years103 | Low rates of heavy infection (note: different results given in first follow up report)104 | Low rates at baseline and follow up105 | Very low rates of heavy infection at baseline and follow up106 | No hookworm found at baseline, 1% at one year, 2% at two years107 | No participants heavily infected at baseline or follow up108 |
For the other two prominent soil-transmitted helminths, ascaris and trichuris, prevalence was low in the Niger and Malawi studies.109 In Burundi, prevalence of ascaris and trichuris decreased somewhat (though in a few cases there were temporary increases). Data from Burundi are given in the footnote.110
Some of the studies also report results for other indicators of disease such as anemia. We omit discussion of these other indicators because they are more likely to be influenced by external factors than are prevalence and intensity (see our previous review of SCI for discussion of these indicators).
Limitations of the prevalence and intensity study data include:
- Monitoring of selected locations. It appears that, in the Niger and Burundi pilot studies, locations included in the study were selectively chosen rather than selected to be a representative sample of treated areas.111
- Low follow-up rates. Follow up rates were low in two of the three countries (at the first year follow-up, 89% in Niger, 33%-50% in the pilot survey and 53%-80% in the other schools survey in Burundi, and 52% in the first follow up in Malawi).112 To be included in follow up surveys, children must be present in school when the surveys are done.113 If those who are present in school are less likely to be infected than those who are not present, this could lead to overstating the impact of the program. The connection between infection status and absenteeism could be a direct relationship (infection could cause absenteeism) or an indirect one (a third factor, such as poverty, could cause both higher levels of infection – perhaps through poor sanitation infrastructure – and absenteeism). Because the second follow up in Malawi was done as a cross-sectional study among children present in school on the day of the study and we present results for children ages 6-8 only, absenteeism and dropout are less likely to bias the results than in the panel studies.
Results from Yemen
In addition, we have two types of results from Yemen:
- Partial sentinel site data: A report SCI shared with us mentions that initial analysis of sentinel site data from July 2014 in Yemen found that prevalence of schistosomiasis decreased substantially.114 These results only include 2,000 of the 8,000 individuals who were surveyed at baseline and the result noted that "a full round of impact evaluation" would be completed in September 2014.115 We have not seen more details about these initial results or any results from the full round.
- Remapping survey: This study compared the number of districts at high-risk, moderate-risk, low-risk for, and uninfected with schistosomiasis at "baseline" (data collected between 2004 and 2010) and in 2014.116 It found large improvements after 2-3 rounds of treatment.117 It is not clear to us whether baseline and follow up results are directly comparable. Baseline data was collected over several years and details of the methodology used at baseline are not given.
Coverage surveys
SCI has conducted, or worked with partners to conduct, surveys in Côte d'Ivoire (in 2014), Malawi (2012 and 2014), Uganda (2014), Mozambique (2015), Zanzibar (2015), and Zambia (2015) to determine what proportion of people targeted for mass drug administration received treatment.
In each of the surveys, surveyors visited a sample of households and asked children, or their parents on their behalf, whether they received treatment in the most recent MDA. Other survey questions, such as age, gender, where the respondent received the treatment, and why they did not take the drug(s), were often included as well. The methodology used differed somewhat across countries. We have summarized the details of the methodologies used in the studies in this spreadsheet ("Methods" sheet). Key differences in the methods used across countries include:118
- Selection of geographic target area: All of the surveys were limited to specific geographic areas (such as districts). In Uganda, Zambia, and Côte d'Ivoire, these were selected randomly or nearly randomly. In Malawi (both 2012 and 2014 surveys), the districts were purposefully selected and not intended to be nationally representative. The selection procedure for Zanzibar was not given in the survey report.119 We are aware of one case, in Mozambique, where a selected village was replaced by another because the surveyors could not locate it; this issue was not mentioned in the survey report.120
- Independence from the government: In Mozambique, the survey was carried out by government health staff, who may have had an incentive to bias the results. SCI told us, "[M]ost of the interviews in one district were done by the other district officers with no connection with the district."121 The reports on the Malawi 2014 and Côte d'Ivoire studies note that the surveyors were independent of the government. SCI told us that university students or staff conducted the other surveys (Malawi 2012, Uganda, Zanzibar, and Zambia).122
- Length of time between MDA and survey: This varied between one and six months. Intuitively speaking, the more time that passes, the less likely children are to remember accurately and the more likely they are to confuse past MDAs (we discuss one case below, from Mozambique, where there may have been confusion been MDAs). Mozambique had the shortest interval at 1-2 months and Zambia had the longest at 5-6 months. Other surveys were generally carried out 2-4 months after the MDA.
- Whether parents or children were interviewed: In Mozambique, parents were interviewed about whether their children took the drugs. In both Côte d'Ivoire and Malawi (both 2012 and 2014 surveys), if children in a household were not available then their parents were interviewed about whether the children had received deworming drugs. SCI made different choices about whether to include these responses in the results, which slightly inflated the results overall.123 SCI told us that parents were not asked to answer on behalf of their children in Uganda or Zanzibar.124 The report on the Zambia survey does not mention adults answering for children.
In addition to limitations in specific surveys, we note some cross-cutting limitations to the methods used:
- Use of verification methods: In Côte d'Ivoire, Malawi (2014), Uganda, Zanzibar, and Zambia participants were asked a number of questions about the treatment program, such as whether they recognized pills or dose poles presented by the interviewers, what they thought of the pills (praziquantel is very large and tastes bitter) and how many pills they took.125 Answers to these questions were not recorded in Côte d'Ivoire,126 and we do not know if they were recorded in the other surveys. We believe that the answers to questions such as these would provide additional evidence about the quality of the coverage results and it is unclear to us why SCI has not recorded, or if it has recorded it, why it has not shared this information. In Mozambique, respondents were asked whether they recognized the dose pole used in schistosomiasis MDAs. However, in that survey parents were surveyed on their children's behalf127 and most children (79%) received drugs at school,128 presumably when parents were not present. We don't know how to interpret the result that a very high percentage of parents (median 90%, ranging 61-94% across provinces) reported recognizing the dose pole.129 SCI hypothesized that parents may either recognize the dose pole from publicity efforts prior to the MDA or remember a similar dose pole from previous MDAs for lymphatic filariasis.130 In either case, this may indicate that the coverage survey is not measuring actual delivery of drugs to children in the most recent MDA.
- Accuracy of responses from young children: SCI told us, "It can be difficult to get clear, accurate answers from young children (5-6 years old). Children, especially younger ones, may be influenced by others who are around during the survey. This is especially so because surveyors often interview older children first, in front of younger siblings."131
- Supervision and auditing of surveys: There is no mention in the coverage survey results of any re-surveying of households to check the accuracy of the data collected and, although "supervisors" are mentioned in several reports, it is not clear what role they played.132 SCI described to us the supervision used in the Mozambique survey (details in footnote); audits were not mentioned.133
The fact that the surveys identified low coverage in several cases increases our confidence in their reliability. Given the smaller sample size, government involvement in the survey, and question about parents recognizing the dose pole noted above, we are more skeptical about the results from Mozambique than those from other countries.
Mass drug administration coverage among school-aged children
| Survey | Median PZQ coverage and range | Median ALB coverage and range |
|---|---|---|
| Malawi (2012) | 77% (64%-90%) | 59% (33%-85%) |
| Malawi (2014) | 69% (55%-77%) | 44% (25%-77%) |
| Côte d'Ivoire (2014) | 82% (67%-88%) | 82% (68%-89%) |
| Uganda (2014) | 47% (24%-86%) | N/A |
| Mozambique (2015) | 81% (73%-89%) | N/A |
| Zambia (2015) | 93% (89%-94%) | N/A |
| Zanzibar (2015) | 80% (75%-85%) | 87% (84%-89%) |
Notes about these results:
- Results broken down by district (or similar geographic region) are in this spreadsheet.
- PZQ is the drug used to treat schistosomiasis. ALB is the drug used to treat STH.
- Ranges and medians are calculated from district-level results.
- The results are for school-aged children only. Some of the surveys also measured coverage rates in adults, who are targeted for treatment in some SCI-supported programs.
- The results exclude districts in Uganda that were included in the survey but which do not receive support from SCI.134
- For context, the World Health Organization recommends that treatment programs aim for coverage rates above 75%.135
Are SCI's monitoring results representative of its work overall?
We have now seen recent monitoring results from about half of the countries in which SCI works, including the five countries were SCI has delivered the largest number of treatments. For those countries from which we have seen monitoring results, we have generally seen one year of results, though SCI has worked in the country for several years.
Details in this spreadsheet.
For countries or years for which we have not seen monitoring data, it is generally unclear to us whether SCI collected additional monitoring data that it has not shared with us or whether it did not collect monitoring data. SCI told us that it is sometimes unable to share results because third parties (e.g. governments, WHO, funders) often need to give permission before data can be shared and because it can take some time for data, once collected, to reach SCI because in some countries it is cleaned and analyzed by country program staff before being shared with SCI.136
For Mozambique, one of SCI's largest recipients of both restricted and unrestricted funds, SCI shared a report from a consultant who visited the country in May 2015 to assist with data cleaning and analysis for prevalence data from 2012, 2013, and 2014. The report notes major problems with this data and refusal of the government to allow SCI to have access to the data outside of Mozambique.137
Additional academic evidence
To provide additional information on SCI's track record, in 2014, we conducted a search for published papers on treatment coverage rates and schistosomiasis and STH prevalence and intensity in countries where SCI has worked.
We focused on papers by Melissa Parker and Tim Allen, who were funded by the Bill and Melinda Gates Foundation to provide an anthropological perspective on SCI's work,138 papers cited in papers by Melissa Parker and Tim Allen, and other papers we identified on this topic from a Google Scholar search.139
The papers we identified were all from Tanzania, Uganda, and Zanzibar, perhaps because these are places that Melissa Parker and Tim Allen's work has focused on.
This spreadsheet summarizes the papers we considered. We have not fully vetted these studies. The studies were generally designed for purposes other than to evaluate SCI's programs so in many cases there is uncertainty about SCI's role in the areas studied. In the discussion below, we have excluded studies that we do not believe were conducted soon after treatment programs in areas targeted by SCI-funded programs.
SCI staff and/or SCI funding were involved in many of the studies.140
It is difficult to draw any conclusions from these studies because of small sample sizes and lack of clarity on SCI's role in each location. In summary:141
- Tanzania (excluding Zanzibar): Two studies at the district level, Stothard et al. 2013 and Chaula and Tarimo 2014, show relatively low schistosomiasis prevalence after treatment (4% and 15% respectively; the latter claims that prevalence pre-MDA was 30%). SCI was working in Tanzania at the time of both studies, but it is not clear if SCI was working in the specific areas studied. Chaula and Tarimo 2014 also shows low treatment coverage (around 40%), though the researchers asked in 2013 about treatment provided in 2011 and 2012.
- Zanzibar: All studies were conducted on Unguja, "the largest and most populated island of Zanzibar."142 Two studies, Stothard et al. 2009 and Rudge et al. 2008, each in a single school, found high prevalence of schistosomiasis in areas that had received treatment (50% and 65% prevalence, respectively). The sample sizes were small, it was not clear why these particular schools were selected, and, while SCI was working in Zanzibar at the time of both studies, but it is not clear if SCI was working in the specific areas studied. Another study, Knopp et al. 2009, in two schools in an area that had received treatment (but perhaps not from SCI) found moderate prevalence of various STHs (21% prevalence for hookworm and low infection intensity). The schools were selected because they had been surveyed in 1994, when prevalence was found to be much higher.
- Uganda: We reviewed three studies of schistosomiasis prevalence: Muhumuza et al. 2013 was conducted in part of a district that seems to have received several rounds of treatment (but perhaps not from SCI). Brooker et al. 2005 was conducted across a district that had its first MDA the year before, which was funded by SCI. Standley et al. 2009 was conducted across six districts, one district that had never been treated (but from which only one school, which had low prevalence, was included in the analysis), two districts that seem to have been treated only once, and three districts that seem to have been treated for many years by SCI. Standley et al. 2009 explicitly aimed to "ambush" schools that might not have been reached by treatment programs.143 Each study found moderate to high prevalence of schistosomiasis (Muhumuza et al. 2013: 35%, Brooker et al. 2005: 28%, and Standley et al. 2009: 42%). Muhumuza et al. 2013 and Standley et al. 2009 found fairly high infection intensity (116 and 634 average eggs per gram respectively among positive cases; the WHO threshold for "high intensity" is 400 eggs per gram144 ). Muhumuza et al. 2013 found 28% coverage in the most recent round of treatment. The coverage survey in Muhumuza et al. 2013 seems to have been six months after treatment.
Possible negative and offsetting impact
- Concerns over whether treatment was sustained: We believe it is important that deworming programs are sustained over time, as re-infection is rapid and a one-time treatment may have little long-term effect.145
It is not clear to us the extent to which SCI-funded programs have succeeded in treating the same children multiple times, as opposed to simply treating the same areas multiple times (and thus treating different children once each).
We remain unsure about how many treatments are needed to impact health. SCI told us that its views on what groups should be treated and how often "is largely based [on] WHO recommendations, but also on government wishes and on intuition and common sense, though it usually works and SCI collects sufficient data to know when it isn't working. In general, in high endemicity areas re-infection is a major issue; in lower endemicity areas, a single treatment can be sufficient."146 One example of the variation in treatment patterns is what SCI told us about its program in Yemen:
SCI distinguishes between high, medium and low prevalence areas. In high prevalence areas, SCI treats the whole population once, and children for five years. In medium prevalence areas, SCI treats the whole population once, and children every other year. In low prevalence areas, SCI treats children every other year.147
- Displacement of government funding for deworming: This could be a concern if, due to SCI's spending on national deworming programs, government funds that otherwise would have been spent on deworming are spent on other, less worthwhile budget items. In the past, SCI has largely supported programs that did not exist before its support.148 We have not seen data on government spending on NTDs before and after receiving SCI support. Ethiopia's Neglected Tropical Diseases Program Manager told us that the government had not dedicated funding to schistosomiasis and that without SCI's involvement the program would likely not have gone forward.149
- Diversion of skilled labor: Drug distribution occurs only once or twice per year and appears to be conducted by teachers, community drug distributors (who receive minimal training to fulfill this role), and health center staff.150 Given the limited time and skill demands of mass drug distribution, we are not highly concerned about distorted incentives for skilled professionals.
- Popular discontent: We have heard a couple accounts of discontent in response to SCI's mass drug administration campaigns, including one case that led to riots.151 SCI notes that following episodes of popular discontent, it has worked with governments to improve public education about the programs.152
What do you get for your dollar?
We estimate that on average the total cost of a schistosomiasis treatment delivered in SCI's programs is $1.26. Excluding the cost of drugs (which are often donated) and in-kind government contributions to the programs, we estimate that SCI's cost per treatment is $0.53. There is significant uncertainty around this number. As discussed above, the information we have seen on SCI’s expenses is limited and possibly unreliable. Similarly, we are not confident in the accuracy of the data we have seen on number treatments delivered. Given this, we make a number of assumptions and judgments in interpreting the data that we have seen and this could introduce errors (which could potentially overstate or understate the actual cost, though we generally try to conservatively err on the side of counting fewer treatments and more costs).
In 2014, SCI estimated its cost per treatment at $0.80.153 As of October 2015, SCI estimates that after April 2016 its cost per treatment excluding costs for drugs and costs paid for by governments will generally be about $0.30.154 We are unsure how it calculated these estimates. In September 2015, SCI told us that it expects to improve its cost-effectiveness analysis by the end of the year.155
We discuss how the cost per treatment figure relates to how much it costs to improve a child's health and development at our report on mass treatment programs for schistosomiasis and STHs.
The remainder of this section discusses our cost per treatment analysis. Our calculations and sources are shown in more detail in this spreadsheet. We also discuss the prevalence and intensity of disease in the places SCI works, which we use to adjust our estimate of SCI's cost-effectiveness compared to the cost-effectiveness of the best-studied deworming programs.
In 2014, we estimated that on average SCI delivers a schistosomiasis treatment for $1.23. The main changes since last year's estimate:
- DFID began providing funding for programs in Ethiopia and DRC in the 2014-15 budget year and we have added the costs of these programs (starting in April 2013156 ) and number of treatments delivered to our estimate.
- We added treatments and costs for the 2014-15 budget year.
- As discussed below, we discounted the number of reported treatments by 10%.
- We added an estimate of costs paid by Imperial College (e.g., office space and some legal and administrative expenses). We increased SCI's costs by 10% to account for this.
Our approach
Our general approach to calculating the cost per treatment is to identify comparable cost and treatment data and take the ratio. We prefer to have a broadly representative selection of treatments in order to mitigate possible distortions, such as using data from a new program, which may incur costs from advocacy, mapping, etc. before it has delivered any treatments.
It is our understanding that SCI intends to treat for STHs in all places where it treats for schistosomiasis, so the treatments SCI reports can generally be interpreted as combination schistosomiasis and STH treatments,157 though we are aware of several cases in which schistosomiasis-only treatments were delivered either by design or due to problems with implementation.158
To get the total cost, we attempt to include all partners (not just SCI) such that our cost per treatment represents everything required to deliver the treatments.159 In particular, we include these categories:
- SCI’s funding to country programs (e.g. to fund drug delivery).
- SCI’s headquarter costs (e.g., for management and technical salaries), including an estimate of costs paid by Imperial College (e.g., office space and some legal and administrative expenses).
- Cost of drugs. We include the full market cost of all praziquantel that is needed to deliver the treatments, regardless of whether SCI purchased it or used donated drugs.
- Costs incurred by the government implementing the program (e.g. for staff salaries when working on treatment programs).
SCI notes that cost per treatment calculations should include sensitivity analysis160 – analysis on the degree to which the cost per treatment varies when various assumptions vary. We have not yet completed such an analysis.
Our analysis
We analyzed several sources of data, which cover different time periods, and developed a several estimates, two of which we summarize here. Full details in this spreadsheet.
- SCI’s recent programs: $1.26 per treatment. The ICOSA program (the name for SCI's DFID-funded work) covers eleven country programs and has been funded primarily by SCI’s first DFID grant, with additional funding from both restricted and unrestricted sources. We have seen data that we think provide a relatively comprehensive picture of spending and treatments over the first five years of the program (October 2010 - March 2015). We have not included the cost of research programs (which are funded separately) in these countries. It is possible that some of this research funding contributed to the treatments we are counting. A more conservative estimate, including about $1.8 million of research expenses in the same countries, is $1.32 per treatment.
- SCI’s early programs: $1.46 per treatment. SCI previously shared with us a summary of the treatments it delivered and the costs it incurred during its early programs (from about 2003-2009). There is some ambiguity in the treatment data that we have interpreted conservatively (in other words, this estimate may be too high, as described in the footnote).161
Note that these estimates are in nominal dollars – we have not adjusted for inflation.
Shortcomings of our analysis
While we believe the estimate described above is reasonable, we want to highlight specific reasons to interpret it with caution.
We rely on reported treatment data. Our understanding is that these data can overstate treatments, so we have discounted this data (by 10%) based on the differences between reported treatment rates and treatment rates found in the coverage surveys discussed above (see footnote for why this is an imperfect comparison).162
We rely on an estimate that 30% of overall program costs are attributable to the government. We derived this from an analysis of a single program in Niger (this footnote elaborates on the details and concerns).163
We do not have data that indicate what proportion of drugs are wasted. We expect that in some cases drugs are purchased or donated but expire before use. We do not know how common this is. In our analysis, we have assumed that 10% of drugs are wasted, which increases the cost per treatment by about $0.05.
We do not have data on Imperial College's expenses that support SCI. Based on a conversation with SCI, we have roughly estimated this support as 10% of SCI's expenses (excluding drugs and government contributions).164
We simply estimate an average cost across programs and do not account for variations in different contexts. SCI told us that costs can vary significantly, for example, due to increased transportation costs in some contexts.165
Baseline infection status
SCI's current and future programs may be less cost-effective than past programs or than programs discussed in our report on deworming because of lower baseline infection rates in current and future programs.
In 2014, SCI shared baseline data from countries it had recently started work in. We compare these rates to rates observed in the best evidence for the effectiveness of deworming, in order to understand how similar SCI's impact is likely to be to that observed in the studies. Schistosomiasis and STH prevalence and intensity in these countries was generally fairly low compared to the studies providing the best evidence for the benefits of deworming (Bleakley 2007, Croke 2014, and Miguel and Kremer 2004) and compared to some of SCI’s earlier prevalence and intensity studies (from Burkina Faso, Uganda, Niger, and Burundi).166
For the most part, baseline data was collected in schools that had been selected for prevalence and intensity studies. The baseline reports use methodologies that seem similar to the other SCI panel studies discussed above. With the exception of the study discussed above from Malawi, we have not examined how representative these schools are of the full treatment area or fully vetted the methodology used. For Ethiopia, we have used data collected during disease mapping and made several assumptions to make that data comparable to the data from other countries.167
In Malawi an error in data collection may have resulted in prevalence being underestimated.168 In Zanzibar, treatment has been ongoing,169 so the study does not reflect pre-treatment conditions.
Detailed results and sources in this spreadsheet.
Is there room for more funding?
In short:
- Estimated needs: SCI estimates that it would use the following amounts of unrestricted funding in each of the next three years (in millions of US dollars):
- April 2016- March 2017: $9.5
- April 2017- March 2018: $13.6
- April 2018- March 2019: $13.3
- Cash on hand: SCI currently has relatively limited unrestricted funding available. Our best guess is that, excluding any additional funding that it might raise before that time, SCI will hold approximately $1.7 million as of April 2016 (the start of its next fiscal year) that it could allocate to program implementation. In addition, it will hold approximately $662,000 and 2 years worth of staff salaries in reserve.
- Other sources of funds: Our impression is that GiveWell-influenced donors contribute most of SCI’s unrestricted funds. As a result of the funding it has received due to GiveWell's recommendation, SCI has not to prioritized fundraising. After SCI set its fundraising targets, a funder committed $2 million per year for three years for the Ethiopia deworming program.
- Past spending: SCI has allocated all of the unrestricted funds it had received by April 2015 (including $6.4 million from GiveWell-influenced donors in 2014170 ), and expects to have spent these funds by April 2016. We have relatively limited information about whether it has continued to spend additional funds in a cost-effective manner, particularly in the past year when it received a significant increase in unrestricted funds.
- Additional considerations: We have continued to face communications challenges with SCI that reduce our confidence that we have a complete, accurate understanding of SCI’s financial situation. Also, the plans SCI shared with us at the end of 2014 did not match its eventual use of the funds it received and it is unclear to us what caused the shift (more in our August 2015 update).
Details follow.
Sources of uncertainty
Overall, there is significant uncertainty in our expectations of how much additional funding SCI could use and how additional funding would be spent. We believe this is primarily due to SCI having limited ability to predict the opportunities it will have in the future because of quickly changing circumstances in many countries and our relative lack of understanding about how SCI has spent funds in the past and why its plans have changed. Country programs may face many different non-funding related constraints, and these seem hard to predict. For example, political unrest delayed the program in Côte d'Ivoire for 18 months,171 in 2014 SCI was not yet ready to allocate additional funds to Mozambique because of lack of confidence in the program's ability to scale further at that time,172 and the Ebola outbreak has delayed work in Liberia.173 Factors that can shift SCI’s planned uses of unrestricted funding include political unrest, expiring drug supplies, additional donated drugs becoming available, delays and budget changes due to coordination with other actors, results of disease mapping, and grants from other donors.174
Challenges communicating with SCI on its room for more funding may also be contributing to our uncertainty. In the past, our understanding was developed largely through conversations with SCI's leadership, supplemented with details from many other sources. In retrospect, our understanding of how SCI planned to use funds often did not match how SCI decided to allocate funds the next time it set program budgets.175
This year, we have relied primarily on information from SCI about how much total unrestricted funding it aims to raise and how it would spend this funding. We have limited information on:
- How SCI will prioritize opportunities if it receives less than its fundraising goal. We have not attempted to learn more about this because our understanding is that SCI's budgeting process is based on meetings with program managers in the first few months of the year and it is difficult for SCI to predict how programs will be prioritized ahead of time.
- How SCI would use funding that exceeded its fundraising goal.
- How likely it is that each country program might face non-funding constraints to scaling up or, in the case of Nigeria, to starting a new program. SCI has taken initial steps toward starting a program in Nigeria. SCI attended a meeting in June 2015 in Nigeria to discuss the possibility of SCI working in the country.176 SCI told us that, more recently, leaders from several Nigerian states have approached SCI to request its assistance starting deworming programs.177
- Other potential funders. SCI has applied for a $500,000 grant for its work in Malawi and a £100,000 (about $150,000) grant for its work in Madagascar.178 Beyond these grants, it is our understanding that SCI does not have major funding prospects for the next year, but that existing funders could make gifts that would reduce its room for more funding.179 In the past, SCI has not actively fundraised from corporate or individual donors, but it is considering doing more by hiring someone to work on this or working with Imperial College's fundraising team.180 GiveWell-influenced donors contribute most of SCI’s unrestricted funds.181 In 2014, we tracked about $6.4 million donated to SCI as a result of our recommendation.182 SCI's draft financial statements for April 2014 - March 2015, state that SCI raised about $7.2 million in unrestricted funds in that period.183 As we discuss above, we have concerns about the accuracy of these financial statements.
In addition, as of October 2015, SCI reported a $2.22 million funding gap in Ethiopia for the budget year 2016-2017, a $2.96 million gap for 2017-2018, and a $3.06 million gap for 2018-2019.184 Since then, a funder committed $2 million per year for three years to the Ethiopia deworming program. The grant is not to SCI and SCI notes that the uses of this funding may not fully overlap with its planned activities. SCI also notes that it still aims to reach its previously stated fundraising goal because this would give it some more flexibility. For example, it is interested in spending $1 million to purchase schistosomiasis drugs for adults in Ethiopia.185
Uses of additional funding
SCI aims to raise $9.5 million for its April 2016 to March 2017 budget year (this figure does not appear to take into account unallocated funds that SCI currently holds; more below). SCI has $7.4 million in restricted funds committed for that budget year from DFID, the END Fund, and other donors, so in total it aims to have a budget of $16.9 million. SCI projects that it would deliver 55.1 million treatments with a budget of this size. This is an increase over the 42.8 million treatments SCI expects to deliver in April 2015 to March 2016.186
Additional funding would support programs in 15 countries. SCI has previously supported programs in 14 of these countries. It has not yet worked in Nigeria. Five country programs would receive 81% of the additional funding: Ethiopia (24%), Mozambique (21%), Sudan (14%), Nigeria (13%), and Malawi (9%).187
Full breakdown of how SCI would spend additional funding by country is in this spreadsheet.
SCI told us that if it does not fully close its funding gap the first thing it would cut would be support for a new program in Nigeria. If it were to raise more than $9.5 million, it might have opportunities to support new programs in additional countries, for example in Chad.188
SCI aims to continue to expand its programs between April 2017 and December 2019 and has a goal of delivering at least 300 million treatments between 2010 and 2019. To do so, it estimates that it will need to raise an additional $13.6 million to support programs for April 2017 to March 2018 and $13.3 million for April 2018 to December 2019.189
Available unrestricted funding
We do not know how much unallocated, unrestricted funding SCI currently holds. We guess that, in the absence of a renewed GiveWell recommendation in late 2015, it would have very roughly $1.8 million to allocate for its April 2016 to March 2017 budget. This guess is based on (a) SCI telling us in early 2015 that it expected to spend all unrestricted funds it held as of that time by the end of the budget year,190 and (b) a rough estimate that SCI will receive at least $1.7 million in unrestricted funds between April 2015 and March 2016.191 We also estimate that SCI will receive very roughly $0.7 million in unrestricted funds from donors not influenced by GiveWell's recommendation before the start of the next budget year.192 Starting in April 2016, SCI may begin holding some unrestricted funds in reserve to help sustain programs in the event that its revenue decreases. It expects to allocate one month's worth of expenses (based on 2014-2015 spending), about $662,000, to this reserve,193 leaving very roughly $1.7 million available to allocate to programs.
As discussed above, a funder has committed $2 million to the deworming program in Ethiopia for 2016 (and the following two years). We subtract this funding from SCI's room for more funding for the next budget year because we would guess that most of it will be used to fund activities that overlap with the activities SCI was planning to fund, though we are not confident in this interpretation and SCI disagrees with it to some extent (see previous section).
We therefore estimate that SCI has about $5.8 million ($9.5 million minus $1.7 million minus $2 million) in room for more funding for its next budget year.
Global need for treatment
There appears to be a substantial unmet need for schistosomiasis treatment globally.
SCI shared an unpublished World Health Organization (WHO) estimate of the number of school-aged children and adults who require treatment for schistosomiasis and those who received treatment in 2014. We do not have permission to publish this data, but we note that only a small portion of those who WHO believes need treatment received it in 2014.194
SCI as an organization
- Track record: SCI has consistently gotten national deworming programs to go through, as discussed above. We know fairly little about how effectively these programs have delivered treatments.
- Self-evaluation: SCI’s self-evaluation is strong compared to the vast majority of organizations we have considered. That said, this evidence is incomplete and has quite a few limitations. In addition, we have a significantly different perspective than SCI on the strength of the evidential case for deworming (see our 2012 post on deworming and the comments that follow it).
- Transparency: SCI has consistently been strong in its commitment to transparency. It has generally provided the information we’ve asked for and has never hesitated to share it publicly (unless it had what we felt was a good reason). It has allowed a lot of public dialogue that other charities may have been uncomfortable with.
- Communication: We don’t feel that SCI has ever purposefully been indirect with us, but we have often struggled to communicate effectively with SCI representatives, and we still lack important and in some cases basic information about SCI's finances. We find this problematic given the amount of effort we have put into understanding SCI's finances.
More on how we think about evaluating organizations at our 2012 blog post.
Sources
{kind=link}
- 1
"Objectives of SCI
- To encourage development of sustainable schistosomiasis and STH control programmes in sub-Saharan Africa.
- In the selected countries: to reach at least 75% of school-aged children (which in most countries would be from 6 to 15-year-old) and other high-risk groups with chemotherapy, namely PZQ and ALB; and thereby reducing prevalence and intensity of schistosomiasis and STH infections; as well as reducing schistosomiasis-related morbidity in high risk groups; and burdens due to STH infections in the targeted populations.
- To create a demand for sustained schistosomiasis and STH control.
- To promote access to anthelmintic drugs and good case management in the regular health system.
- To develop a rigorous monitoring and evaluation plan which will generate the information required to determine whether or not the objectives have been met."
Fenwick et al. 2009, Pg 3.
- 2
"The move towards national control programmes in sub-Saharan Africa was facilitated by an award from the Bill and Melinda Gates Foundation (BMGF; http://www.gatesfoundation.org) Global Health Program in 2002, to the SCI for the implementation and evaluation of control of schistosomiasis." Fenwick et al. 2009, Pg 2. Amount at Gates Foundation, Imperial College London (June 2002).
- 3
"Six countries were selected by October 2003 for full support: Burkina Faso, Mali, Niger, Uganda, Tanzania and Zambia. The countries each proposed a different implementation approach and management structure for their large-scale schistosomiasis control. This was readily accepted because the BMGF required SCI to test the ‘proof-of-principle’ of national scale, Ministry of Health (MoH)-led schistosomiasis control programmes. SCI is based in Imperial College London and operated with the principle that all programmes were country owned and run, with SCI staff offering technical and other assistance, but not as expatriates living in-country. Programmes were based in the MoH in the respective country, and SCI offered support to improve the national health system." Fenwick et al. 2009, Pg 2.
Between 2003 and 2008, SCI provided treatment for schistosomiasis and soil-transmitted helminths to the following number of people (Fenwick et al. 2009, Pg 3, Table 1).
Number treated by country (millions) Year Uganda Burkina Faso Niger Mali Tanzania Zambia 2003 0.43 - - - 0.10 - 2004 1.23 1.03 0.67 - 0.44 - 2005 2.99 2.30 2.01 2.60 2.95 - 2006 1.51 2.82 1.56 2.18 0.38 0.56 2007 1.81 0.75 2.07 0.65 2.65 0.25 2008 1.50 2.70 5.28 - 1.24 - - 4
- "Current and future rounds of treatment in all six countries are being delivered in an integrated manner to include schistosomiasis, STH, lymphatic filariasis, onchocerciasis and trachoma." Fenwick et al. 2009, Pg 10.
- The "six countries" refers to the six countries funded by SCI's first Gates Foundation grant.
- Countries and dates from SCI Board management accounts (April 2010)
- 5
SCI Burundi: Impact
SCI Rwanda: Strategy
SCI Board management accounts (April 2010) - 6
- 7
- 8
"A team from Imperial College London has been awarded 25 million funding from the UK Government to continue its fight against neglected tropical diseases, it was announced this week. The money will enable the Schistosomiasis Control Initiative (SCI) to provide 75 million treatments to protect some of the world’s poorest children against schistosomiasis – an illness caused by parasitic worms – and soil-transmitted helminths (STH). £15 million of the funding will be spent directly on procuring drug treatments, through an organisation called Crown Agents. The rest will be administered by SCI." SCI Imperial initiative to protect children from tropical disease awarded ₤25m government backing.
- 9
”DFID has allocated 50 million GBP for control of neglected tropical diseases, of which 25 million is going through SCI for schistosomiasis control in 8 countries (including Malawi) over five years.” GiveWell's notes from visit to Malawi on October 17-19, 2011.
- 10
"SCI will be assisted in their drug delivery by the Centre for Neglected Tropical Diseases at Liverpool School of Tropical Medicine via a subcontract through LATH (Liverpool Associates in Tropical Health). In six countries, this will lead to treatment for lymphatic filariasis – another worm disease – becoming integrated with schistosomiasis and STH treatment." SCI Imperial initiative to protect children from tropical disease awarded ₤25m government backing.
- 11
- 12
As of July 2011, it had received about $580,000 in unrestricted funding (SCI IC Trust summary (September 2011)) and $108 million overall (SCI Gates Foundation final report (January 2011) Pg. 20).
- 13
"For the smaller donor, we have two or three projects, which we have been supporting and which will hopefully lead to pilot project in their respective countries.
- In Côte d'Ivoire, we now have funding from the U.K. Department for International Development (DFID). There will eventually be a national program.
- In Mozambique, we have a doctor running a practice for 70,000 people. We have been funding her to test people, do surveys and give drugs to treat people. Up until now, that has taken all the individual funding that comes in."
Alan Fenwick, SCI Director, phone conversation with GiveWell, February 16, 2011.
- 14
Donations due to GiveWell's research through January 2015 are listed here and total about $10.5 million. In February through August 2015, we tracked about $900,000 to SCI, including funds that GiveWell allocated to SCI from its general regranting funds.
- 15
We estimate that SCI received about $8.6 million due to GiveWell's recommendation between April 2013 and March 2015 (internal data). Over that period, SCI reports $12.4 million in unrestricted revenue. SCI financial statement 2013/14 and 2014/15 (revised October 2015). SCI's total may include some restricted funds. More details here.
- 16
SCI financial statement 2013/14 and 2014/15 (revised October 2015).
- 17
- GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, June 17, 2010.
- SCI Summary sheet of treatments instigated and overseen by SCI.
- SCI Proposal by SCI, Imperial College to manage the Program for Integrated Control of Neglected Tropical Diseases in Côte d'Ivoire.
- Conversations with four program managers, discussed below.
- 18
Sudan
- Sudan NTD concept paper (2015-2018)
- Sudan PZQ and ALB treatments by locality (2015)
- Sudan annual workplan (April 2015 to March 2016)
- Sudan cash book
- Sudan campaign photos
- Sudan annual workplan for WHO (2015)
- Sudan joint request for selected PC medicines
Nigeria
- 19
"Prior to SCI’s work in Côte d'Ivoire, there were no large-scale schistosomiasis (SCH) treatment programs." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 20
"SCI first contacted the government and started to discuss a SCH/STH program in 2010. A civil war delayed progress because there was political turmoil, a weakened health system, and dangerous conditions. In 2012 conditions improved, and the contracts between SCI and the Ministry of Health were set up. [...]
Treatments started in December 2012:- In 2012: 649,859 school-aged children (SAC) received treatments in 12 districts, some of which had been mapped prior to SCI’s involvement.
- In November 2013: 853,708 SAC received treatments in the areas that SCI mapped first, with the help of the Ministry of Health.
- In May 2014: 1,425,461 SAC received treatment in the remaining areas of the first phase of mapping.
- In November 2014: 3.5 million SAC are targeted for the next treatment, which would correspond to the second phase of mapping.
The aim is that by the end of 2014, all SAC in the SCH-endemic districts will have been treated at least once. Some areas that were treated in 2012 were also treated again in May." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 21
"In May 2014: 1,425,461 SAC received treatment in the remaining areas of the first phase of mapping. In November 2014: 3.5 million SAC are targeted for the next treatment, which would correspond to the second phase of mapping." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 22
Alan Fenwick, email to GiveWell, November 3, 2015. Note this is slightly higher than we previously reported in our August 2015 update on SCI.
- 23
"For the smaller donor, we have two or three projects, which we have been supporting and which will hopefully lead to pilot projects in their respective countries.
- In Côte d'Ivoire, we now have funding from the U.K. Department for International Development (DFID). There will eventually be a national program.
- In Mozambique, we have a doctor running a practice for 70,000 people. We have been funding her to test people, do surveys and give drugs to treat people. Up until now, that has taken all the individual funding that comes in."
Alan Fenwick, SCI Director, phone conversation with GiveWell, February 16, 2011.
- 24
SCI planned SCH treatment numbers by country by year (October 2015).
- 25
- Vitol: Côte d'Ivoire mapping; £102,152; grant period: 01/10/2012 to 31/12/2013. (Pg 3). SCI advisory board financial report (June 2014).
- DFID ICOSA £177,000 in 2013-14. SCI advisory board financial report (June 2013).
- DFID ICOSA: £200,000 in year 5 of the grant (Pg 9). (The grant is "A six year contract from October 2010 to March 2016," (Pg 7) and DFID's fiscal year is from April 1 to March (DFID glossary), so year 5 is April 2014 to March 2015.) SCI advisory board financial report (June 2014).
- SCI has reported $525,264 in spending in Côte d'Ivoire from unrestricted funds between November 2011 and September 2014. GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates.
As of November 4, 2014, Google states that £1 is worth $1.6.
- 26
SCI financial statement 2013/14 and 2014/15 (revised October 2015). Note that SCI told us, "SCI used unrestricted funds to conduct a community health questionnaire in areas with low coverage. [...] This questionnaire was the main use of unrestricted funding in Cote d’Ivoire in 2014." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
- 27
"If the 2014 targets are met, it will be an impressive achievement to have treated all SCH-endemic areas at least once since 2012. With just the funding allocated by DFID, the program could not have scaled up as quickly. In this scenario, it probably would have completed the mapping but delivered fewer treatments." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 28
- "SCI conducted national mapping since late 2012, finishing in March 2014. In total, all 82 districts in Côte d'Ivoire were mapped. This was done in two phases because of limited funding. The first phase was done by the Ministry of Health with support from SCI. The second phase was led by Professor Eliézer N’Goran from the Université Félix Houphouët-Boigny with both technical and financial support from SCI. […]
The country will start an integrated treatment program for several diseases in November 2014 […]
Other neglected tropical disease (NTD) organizations have benefitted from the work SCI has done to build a SCH program. SCI has provided cars and developed staff capacity. Organizations have worked to coordinate when sharing these resources and operating an integrated program should make that easier." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014. - "Cote d’Ivoire is working toward creating an integrated program for the treatment of lymphatic filariasis, onchocerciasis, schistosomiasis, and STH. This will involve collaboration and integration of tools and training, but drugs for all four diseases will not be administered simultaneously. So far, lymphatic filariasis and onchocerciasis treatments have been integrated, and schistosomiasis and STH treatments are administered together but currently delivered separately from lymphatic filariasis and onchocerciasis. [...] SCI's partners in Cote d'Ivoire include Sightsavers, the END Fund, and Helen Keller International." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
- "SCI conducted national mapping since late 2012, finishing in March 2014. In total, all 82 districts in Côte d'Ivoire were mapped. This was done in two phases because of limited funding. The first phase was done by the Ministry of Health with support from SCI. The second phase was led by Professor Eliézer N’Goran from the Université Félix Houphouët-Boigny with both technical and financial support from SCI. […]
- 29
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 30
"Dr. Nogaro has visited Côte d'Ivoire several times over the last year, often dealing with multiple activities on each trip:
- One month last November to oversee the sentinel sites activity and obtain baseline information for both prevalence and intensity of infection, help with the MDA, and oversee the start of the second phase of mapping,
- One month in January to work on the coverage survey, work on financial reporting, oversee mapping, and help with drafting the annual work plan and budget (alongside the Ministry of Health),
- Three weeks in May for another MDA,
- One week in June to work with WHO and other partners for the integrated MDA plan and budget work, and
- Three weeks this month to follow up with CHWs in low coverage areas, oversee the sentinel sites activity, and oversee the first integrated MDA and training."
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 31
"Program staff in each country create annual budgets in collaboration with SCI. The budget ensures money is being spent well and on activities defined in the annual work plan, which is submitted by the country to SCI. Generally, receipts are used to document expenses. In some cases, it takes a long time to get the receipts or receipts are not available at all. SCI hired an accountant and an auditor to better monitor finances." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 32
"Data is entered at the country level. For example, data from mapping and sentinel sites can be handled by students at a local university. The data is double entered to ensure accuracy. The original forms stay in the country and the database is sent to SCI, which can then run analyses. SCI is planning to expand its data analysis team. In the spring, SCI’s biostatistician will teach a data cleaning session to program staff in Côte d'Ivoire. In the future, SCI will consider doing more advanced data analysis training in all the countries it supports." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- 33
"In 2007, prior to SCI’s involvement, Save the Children ran a one-time treatment for about 1 million children for schistosomiasis (SCH) and soil-transmitted helminths (STH)." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 34
"In mid-2012, the University of Gondar invited SCI to an international symposium on SCH, which served as an introduction for SCI to Ethiopia. After this, Dr. Fenwick, Director of SCI, and other senior SCI staff established a relationship with senior Federal Ministry of Health (FMOH) officials.
In 2013, SCI moved into more serious conversations with the Ministry of Health. In July 2013 SCI provided support for the launch of the FMOH’s National NTD Master Plan at an international symposium in Addis Ababa. Around the same time, SCI collaborated with the Ethiopian Health and Nutrition Research Institute (EHNRI; now renamed as the Ethiopian Public Health Institute), the technical arm of the FMOH, to plan and fund nationwide mapping. […]
Last year (2013) SCI funded 1.4 million combined SCH/STH treatments. […]
The mapping took longer than planned. Teams were trained in November 2013, and the mapping was completed in April 2014." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014. - 35
SCI Ethiopia treatment campaign summary report (April 2015).
- "In total 2.9 million school-aged children received treatment against both schistosomiasis and STH (coverage of 74.0%),comprised of 2.3m enrolled SAC and 571,000 non-enrolled. These numbers are currently being validated using coverage validation surveys in representative districts. These results will be presented as soon as the data is analysed." Pg 1.
- "Demographic and parasitological data were collected from 22 sentinel sites prior to the April 2015 campaign. Each sentinel site comprised of a school, with 125 children recruited from each school. Each child provided stool and urine samples on two consecutive days in order to estimate the level of parasite prevalence and average intensity of infection. These 22 sentinel sites will be supplemented by a further 15 sites prior to the October 2015 round of treatment to complete the picture on the baseline level of infection. These schools will be followed up annually, just prior to treatment, to understand changes in infection across the course of the programme." Pg 4.
- 36
SCI report to DFID (September 2015), Pgs 12-13, Table 2.
- 37
SCI planned SCH treatment numbers by country by year (October 2015).
- 38
Alan Fenwick, email to GiveWell, September 28, 2015. We are not confident that this is a complete accounting of all of SCI's spending on the Ethiopia program. It spans February 2012 to September 2015. Sum cited here includes unrestricted funding only.
See also GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates. We discuss SCI's work in Ethiopia in our November 2012, October 2013, and June 2014 updates on SCI. - 39
Alan Fenwick, email to GiveWell, September 28, 2015. First transfers from END Fund and DFID funds occurred in 2015. Also:
- "Getting sufficient funding from SCI this year was straightforward because it was primarily restricted funding from the END Fund. The first year of this 3-year grant ends in February 2015." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- We note in our June 2014 update on SCI that, as of April 2014, SCI was in the final stages of negotiating the grant from DFID that includes funding for Ethiopia.
- 40
"He does not know if The END Fund/DFID would have gotten involved without the mapping data. At a minimum, the mapping effort significantly increased the probability of attracting external funding and accelerated the program by a few years." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 41
"FMOH [Federal Ministry of Health] began working with SCI about 2.5 years ago. Mr. Shafi's predecessor began speaking to SCI about the possibility of working together on a schistosomiasis program. SCI was the only organization that the government spoke to about this, as it wasn't aware of any other organizations working on schistosomiasis. [...]
Without SCI's involvement, the program would likely not have gone forward. With the exception of filling small funding gaps on an ad hoc basis, the government has not been able to allocate funding to NTDs. It was interested in doing disease mapping but did not have the funding to do so, and it likely would not have received drug donations without the mapping data." GiveWell's non-verbatim summary of a conversation with Oumer Shafi, November 4, 2014. - 42
"In July 2013 SCI provided support for the launch of the FMOH’s National NTD Master Plan at an international symposium in Addis Ababa. Around the same time, SCI collaborated with the Ethiopian Health and Nutrition Research Institute (EHNRI; now renamed as the Ethiopian Public Health Institute), the technical arm of the FMOH, to plan and fund nationwide mapping. […]
The Deworm the World Initiative (DtWI) will be providing technical advice to Ethiopia, based on its experience in Kenya. […]
With funding from Dubai Cares, the Partnership for Child Development (PCD) implemented a small pilot program in 30 schools in the southern region (SNNPR) to look at feasibility of a comprehensive school health and nutrition program, which includes deworming, nutrition, and WASH [water, sanitation, and hygiene] interventions and home-grown school-feeding. Related to this, the grant included funding for a region-wide situational analysis, covering an area with about 17 million people. Therefore, the decision for this to be included in the broader national mapping and to include the distribution of SCH, STH, WASH facilities, and school-feeding needs. SCI and PCD partnered on the design, implementation, and analysis of this national mapping. Overall, PCD provided both technical assistance and about 20%-25% of the funding for the national mapping." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014. - 43
"Examples of Dr. French's work to assist the Ethiopia program:
- Initial program setup activities: creating processes and scheduling meetings to lay groundwork for future activities; developing and finalizing contracts between funders, Imperial Collage [sic] and implementers (the contracts are more complicated than normal because there are 2 funders and 2 implementing agencies).
- SCH/STH action plan: This will provide a detailed plan for next 12 months and more general plan for 5 years. The FMOH have tasked Dr. French and SCI to drive this this forward, e.g providing an outline that can be adapted by the country.
- Mapping plan: Dr. French was the main technical advisor from SCI. He worked very closely with people from EHNRI to a) write the research protocol, b) advise on the recruitment of trainers, and c) train technicians, d) supervise activities, e) help with data collection and analysis.
- Last year’s mass drug administration (MDA): Dr. French was less involved with the MDA than with the mapping but was involved in developing the plans. The Ministry of Health was responsible for running the program and delegating work to regional governments. It had experience from other mass distribution programs. For technical training, it worked with health workers who already had extensive general experience and then provided NTD expertise largely from WHO guidelines, though SCI provided some technical guidance.
Dr. French has been living in Ethiopia, which has helped him build relationships, enabled him to hear more activity details, and allowed him to provide timely advice. For example, he has stronger relationships with the officials in Ethiopia and a clearer sense of whom to go to for various requests. Also, by being close to the activities, some problems with data flowing back to central level have been clearer, which makes it easier for him to help develop solutions." GiveWell's non-verbatim summary of a conversation with Michael French, October 15, 2014.
- 44
"Mike French, SCI's program manager for Ethiopia, works in the same office as the government NTD program." GiveWell's non-verbatim summary of a conversation with Oumer Shafi, November 4, 2014.
- 45
"Prior to SCI’s involvement in 2010, there was a mapping project in 2008. Dr. Blair does not think there were any schistosomiasis (SCH) treatment programs (other than a small program funded by SCI). If there were, they would have been small-scale." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 46
"The SCH program in Mozambique is run by the Center for Neglected Tropical Diseases (CNTD). Funding for the program is provided to SCI by DFID, and SCI funds CNTD as part of its agreement with DFID." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 47
“When we bid for the DFID grant, I was advised that DFID favored grants that involved partnerships. CNTD does a lot of the work on lymphatic filariasis. DFID was providing 20 million pounds for lymphatic filariasis and 20 million for schistosomiasis. Working with CNTD demonstrated a degree of integration. CNTD does both lymphatic filariasis and schistosomiasis in Mozambique." Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014.
- 48
SCI report to DFID (September 2015), Pgs 12-13, Table 2.
- 49
SCI planned SCH treatment numbers by country by year (October 2015).
- 50
DFID funds:
- DFID ICOSA £649,514 in 2013-14. SCI advisory board financial report (June 2013), Pg 7, “Overseas country budgets - FY4.”
- DFID ICOSA: £150,000 in year 5 of the grant (Pg 9). (The grant is "A six year contract from October 2010 to March 2016," (Pg 7) and DFID's fiscal year is from April 1 to March, so year 5 is April 2014 to March 2015.) SCI advisory board financial report (June 2014), Pg 9.
Unrestricted funds: SCI draft financial statements for 2013/14 and 2014/15 reported that the unrestricted funds SCI spent in Mozambique summed to £595,421 in 2013-14 and £596,588 in 2014-15. SCI later told us that this document may not be accurate. SCI responses to GiveWell questions on financial statements (October 2015).
- 51
"In January 2011, SCI were awarded three SCORE studies
TITLE: Studies of Gaining and Sustaining Control of Schistosomiasis- Study: Schistosoma haematobium: Gaining and Sustaining Control of Schistosomiasis in Capdelgado, Mozambique
- Study: Schistosoma haematobium: Gaining and Sustaining Control of Schistosomiasis in Kollo and Say Districts, Niger
- Study: Schistosoma Haematobium: Gaining and Sustaining Control of Schistosomiasis in Loga District, Niger."
SCI advisory board financial report (June 2014), Pg 16.
As of June 2014, SCI had spent £366,937 of the £368,030 by SCORE, and expected to receive an additional $368,229. SCI advisory board financial report (June 2014), Pgs 4-5. - 52
See our June 2014 update on SCI.
- 53
"SCI and CNTD are working closely with RTI International in Mozambique. This has been a great working relationship. RTI is funding some capacity development around drug logistics. It is working on trachoma; currently, this work is focused on mapping, but it will likely fund treatment when mapping is finished. RTI has staff in-country and reports to SCI and CNTD on issues, which can provide some verification that the program is progressing as expected. The organizations coordinate to ensure multiple sources of funding aren't allocated for the same purpose. For example, RTI emailed SCI and CNTD saying that the government had indicated that it was going to drop the SCH program; the staff from the organizations communicated quickly to sort out the confusion." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 54
"The SCH program in Mozambique is run by the Center for Neglected Tropical Diseases (CNTD). Funding for the program is provided to SCI by DFID, and SCI funds CNTD as part of its agreement with DFID. [...] CNTD will continue to run the mass drug administration (MDA), but SCI has become more directly involved with the M&E as it has the technical expertise to manage these activities." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 55
"SCI’s program in Uganda is fully funded by DFID (other than one use of unrestricted funding, discussed below). SCI had previously worked in Uganda with funding from the Bill & Melinda Gates Foundation. After this funding ended, USAID funded work by RTI International in Uganda. Around 2006, Uganda started an integrated NTD program in districts endemic with more than one NTD. Districts with only schistosomiasis (SCH) were not treated.
When SCI re-entered Uganda, it started SCH programs in the districts not receiving treatment." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014. - 56
See our August 2015 update on SCI.
- 57
SCI report to GiveWell (September 2014), Annex 1.
- 58
SCI planned SCH treatment numbers by country by year (October 2015).
- 59
- DFID ICOSA £138,386 in 2013-14. SCI advisory board financial report (June 2013), Pg 7.
- DFID ICOSA: £58,994 in year 5 of the grant (Pg 9). (The grant is "A six year contract from October 2010 to March 2016," (Pg 7) and DFID's fiscal year is from April 1 to March, so it's our under year 5 is April 2014 to March 2015.) SCI advisory board financial report (June 2014), Pg 9.
As of November 4, 2014, Google states that £1 is worth $1.6.
- 60
"SCI’s program in Uganda is fully funded by DFID (other than one use of unrestricted funding, discussed below)...
In deciding on the budget, there might be some disagreement around whether impact M&E (having sentinel sites) is worth the expense. The government might prefer to provide more treatments. Mrs. Nalule and other researchers argue for the value of M&E.
Last year, M&E funding was augmented by £23,000 from SCI unrestricted funding. Without this, there likely would have been cuts in the number of sentinel schools. This M&E is enabling research to compare different treatment strategies in areas where prevalence is low. DFID was not interested in funding this research." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014.
Note that SCI has only reported $2,220 in unrestricted spending to us in financial reports. GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates. - 61
- 62
"When SCI re-entered Uganda, it started SCH programs in the districts not receiving treatment. Also, in about 30 districts, USAID stopped treating SCH because prevalence dropped below 20%, so SCI supported the continuation of these treatments with an aim towards elimination. […]
Also, SCI is taking over treatment from RTI in a 15 districts that have higher prevalence, and, in these districts, it will treat adults. Since prevalence is over 50%, WHO guidelines say to treat children and high risk adults (e.g. fisherman), though usually programs will just try to treat all adults." GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014. - 63
"In some cases (for example, Uganda and Niger), the government program manager understands SCH well and does not require a lot of technical guidance. [...] Uganda is an interesting example. The program had been relatively straightforward to manage. It is now focusing on elimination, which is unknown territory so will require much more guidance. There is a lot of research to do to determine guidelines for how often to treat." GiveWell's non-verbatim summary of a conversation with Lynsey Blair, October 16, 2014.
- 64
GiveWell's non-verbatim summary of a conversation with Yolisa Nalule, October 14, 2014.
- 65
Kieran Bird, SCI Finance Manager, conversation with GiveWell, October 16, 2014.
- 66
"SCI has also invested in the finance function including a Financial Director with extensive overseas experience to provide appropriate skill sets to support the programme. The roll out of monthly financial reporting is in progress and will aid more effective tracking of the financial performance of each country. Monthly variance analysis is being included as part of the monthly finance meeting with Programme Managers to assist with forecasting and tracking of performance. An assessment tool for countries to report on SCI's programme and financial management is under development and has been piloted. This will allow SCI to receive feedback from countries and identify areas for improvement. [...] SCI's Finance Director is developing a more comprehensive SCI financial strategy that will focus on revenue tracking to be completed by Dec 2015. Finance policies and a reference manual are in development. To assist this SCI will invest in additional Accounting Software that will interface with the Imperial College systems but will allow a greater level of granularity of data and allow reports to be generated in a more timely manner. Resources have been allocated from Imperial College central finance function to assist in the development and implementation of the appropriate software. [...] The new accounting software package will allow for more timely reporting of funds held at any one time. In addition analysis of variance against budget at the country level is also being undertaken to identify areas of opportunity for efficiency. Comparison across countries can also provide valuable data." SCI supporting documents matrix (September 2015).
- 67
"SCI’s finance and operations manager, Blandine Labry, is leaving the organization, and SCI is currently interviewing candidates for her replacement. SCI has hired two new finance staffers, increasing the number of positions on the finance team to four." GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, July 31, 2015.
It is our understanding that Ms. Labry joined SCI in early 2015.
We spoke with Najwa Al Abdallah, SCI's new Finance and Operations Manager on September 8, 2015. GiveWell's non-verbatim summary of a conversation with Wendy Harrison and Najwa Al Abdallah on September 8, 2015. - 68
- In our November 2012 update on SCI (see footnote 1 of that report), we noted inconsistencies in the spending data SCI shared with us. In one case, we asked SCI about a discrepancy we have noticed and SCI's reply was implausible.
- In our next update on SCI, in October 2013, we reported having a fuller view of how SCI had spent funds, though noted a discrepancy in funds held: "We reported (after checking this number with SCI) that as of October 2012, SCI held $2.65 million in unrestricted funds. As part of this update, we sought to understand SCI's use of unrestricted funds between October 2012 and August 2013. SCI told us that it had held $1.96 million in unrestricted funds as of October 1, 2012, about $660,000 less than we previously thought. We have assumed that we miscommunicated with SCI last year; one possibility is that the numbers we received included some restricted funds and we may not have fully excluded all restricted funds in our adjustment. We have used the more recent figure for this update."
- In October 2014, SCI shared reports of spending since our last update and balance of unrestricted funds at the end of the period. Combining these figures with our previously published figure for balance of unrestricted funds as of our last update implied negative revenue over the period. We asked SCI to explain the discrepancy. SCI first told us that the discrepancy was due to counting some restricted funds in the unrestricted balance. At the same time, SCI provided data on unrestricted revenue over the period, giving us a double check on these figures. There was a discrepancy between actual revenue and revenue implied by the starting and ending balances and spending over the period of about £528,000. When we asked SCI about this discrepancy, SCI told us that there was an additional expenditure of £595,420 that was missing from the report previous, as well as a small amount of additional income, which reduced the discrepancy to £11,651.
- In June 2015, SCI shared financial statements for 2013/14 with us that showed no spending in Ethiopia in that year (SCI draft financial statements for 2013/14 and 2014/15). We asked SCI about this because other communications with SCI indicated that SCI had been active in Ethiopia in that year. SCI noted that this was an error and was likely due to confusion by newer staff on how to interpret older financial data: "The three transfers which were made to Ethiopia during 2013/2014 were recorded to the L‐account which is an account the Imperial College currently use to record unrestricted income. In the past however, the L‐account was also used to record expenditures ‐ but later we changed our recording system whereby expenditures were accredited to 'NX' accounts which were created to capture country expenses. Because the transfers went straight from the L account [SCI staff member] did not identify them as being for Ethiopia." Alan Fenwick, email to GiveWell, October 1, 2015.
- 69
- Najwa Al Abdallah, conversation with GiveWell, October 22, 2015.
- "[GiveWell:] Would DFID funds for those countries be included in the financial statements? Are all unrestricted funds for those country programs included in the financial statements?
[SCI:] Yes all income/expenditure is included; the transfer to the Liverpool University is grouped under central costs because the transfer is not split by country." SCI responses to GiveWell questions on financial statements (October 2015).
- 70
"Some of the funds received from End Fund and [donor name], historically were either received by the IC Trust and some income was donated to the college and was accounted for under the L-account (L and IC Trust in the financial statement are accounted for as unrestricted). New agreements with End Fund for Ethiopia and Yemen and [donor name] grant for Madagascar are under the research projects at P-codes (Restricted)." SCI responses to GiveWell questions on financial statements (October 2015).
- 71
Data from:- SCI Niger spending data (October 2011 to May 2013).
- SCI Tanzania spending data (March 2011 to July 2013).
- SCI Uganda spending data (September 2011 to August 2013).
- SCI Malawi spending data (November 2011 to August 2013).
- SCI CNTD spending data (FY2-FY4).
Summarized in: GiveWell analysis of SCI spending under DFID grant.
- 72
Kieran Bird, SCI Finance Manager, conversation with GiveWell, October 16, 2014.
- 73
SCI report to GiveWell (September 2014), Annex 1.
GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates. - 74
- 75
Data from:
- SCI Niger spending data (October 2011 to May 2013).
- SCI Tanzania spending data (March 2011 to July 2013).
- SCI Uganda spending data (September 2011 to August 2013).
- SCI Malawi spending data (November 2011 to August 2013).
- SCI CNTD spending data (FY2-FY4).
Summarized in: GiveWell analysis of SCI spending under DFID grant (updated 2015).
- 76
SCI's summary of active accounts as of June 2014 lists six research grants totaling £2.6 million, or about $4.1 million over 2010-2014. SCI advisory board financial report (June 2014), Pg 5.
- 77
"Once we have people that want to give at least $100,000, we talk to them directly. [...]
Someone wanted to do something special with his money, so we're doing hydrocele surgery in Niger. He gave us $200,000 and we told him we could do ~1000 hydrocele surgeries.Alan Fenwick, SCI Director, phone conversation with GiveWell, February 16, 2011.
Alan Fenwick, SCI Director, phone conversation with GiveWell, September 15, 2011. Note: "SCI generally doesn't do water and sanitation programs because of the expense. In Burundi they're doing water and sanitation programming because they have been successful there with running a program and treating schistosomiasis, but soil-transmitted helminth infections remain persistent." GiveWell's notes from visit to Malawi on October 17-19, 2011. - 78
Tohon et al. 2008. In 2014, SCI sent us a more recent report, SCI Niger panel study 2011. SCI Niger panel study 2011 is our only source of data on the second to fifth year followups. This analysis excludes three of the eight schools that were originally in the study as well as the 56% of participants lost to follow-up in the remaining five schools. Participants who were followed up for some years but lost to follow-up by the end of the study are completely excluded rather than being included in a separate analysis of the earlier follow-ups. The 3 schools were apparently dropped because they were not surveyed in some years:
- "Of these eight sentinel sites, five had data available in all six years of the study up to 2010." SCI Niger panel study 2011, Pg 19.
- "455 out of 1024 (44%) children recruited at baseline from November 2004 to April 2005 were successfully followed up for the full duration of the 6-year sentinel site monitoring." SCI Niger panel study 2011, Pg 25.
For this reason, we feel that the results from SCI Niger panel study 2011 are hard to interpret, and we don't present them here, relying instead on Tohon et al. 2008.
- 79
We have seen two reports on the Burundi study, Styles 2011 and Koukounari 2011, which use different methods of analysis and included different numbers of participants. Which individuals they included in their analyses is not always clear, however the fact they report similar results for prevalence provides some evidence that the results are not highly dependent on these choices. (Both Dr. Koukounari and Dr. Styles are statisticians who formerly worked at SCI.)
- Pilot study: Styles 2011 and Koukounari 2011 have strengths and weaknesses in defining the sample for the pilot study. Styles 2011 includes a much larger number of individuals (Styles 2011, Pg 3, Figure 1b compared to 710 in Koukounari 2011, Pg 7, Figure 2). However, it is unclear whether the individuals in the follow-up were all in the original cohort or whether some were added to the sample later. The two reports indicate different numbers of students included in the study and retraced at each followup. We have seen two explanations for the differences:
(1) "Dr. Koukounari only included students who were in first grade during the first year of the study and who were successfully surveyed every year of the study. In addition to the children counted by Dr. Koukounari, Dr. Styles included students who entered first grade and were added into the study in subsequent years, as well as students who were missing data from some years. Each of these strategies for data analysis has benefits and drawbacks. SCI initially planned to do a cross-sectional evaluation of sixth grade students every year, because each year the current sixth grade class would have received more rounds of treatment over the course of elementary school than the previous year. SCI did not complete this plan, but Dr. Koukounari included the data from the sixth grade students in the baseline data. Dr. Styles did not include this data." GiveWell's non-verbatim summary of a conversation with Giuseppina Ortu on June 20, 2014.
(2) "In addition to the longitudinal studies at each follow-up newly recruited children were added to these surveys. At 1st follow-up (2008) 2288 newly recruited children were added to these surveys with range age: 6-21 years old and median age: 12 years old. Of these 2288, only 210 i.e. (9.18 %), were of age 6 and eligible to be included in the specific cross sectional data analysis. At 2nd follow-up (2009) 2311 newly recruited children were added to these surveys with range age: 5-20 years old and median age: 11 years old. Of these 2311, only 160 i.e. (6.92 %), were of age 6 and eligible to be included in this specific data analysis. Finally, at 3rd follow-up (2010) 2224 newly recruited children were added to these surveys with range age: 6-20 years old and median age: 12 years old. Of these 2224 only 189 i.e. (8.50 %) were of age 6 and eligible to be included in this specific data analysis." Koukounari 2011, Pg 6. Koukounari 2011 notes that it only includes the 20% of participants in the pilot study who were tracked through all follow-ups: "Finally at 3rd follow-up (2010) there were 713 children successfully followed-up (i.e. follow-up rate=19.71%). Longitudinal analyses for the 4 years are presented in the next pages for these 713 children."Koukounari 2011, Pg 6. - Other schools: Koukounari 2011 claims that 5,700 participants were recruited at baseline: "At baseline (2008) there were recruited 5700 children while the follow-up rate one year later was 53.42 % (3045/5700)." Koukounari 2011, Pg 16. Styles 2011 Pg 13, Table 8 claims there were 3,781 participants recruited at baseline. SCI later told us that this may be because Koukounari 2011 included data from a group of students who were surveyed for a concurrent cross-sectional study, which was not completed: "SCI initially planned to do a cross-sectional evaluation of sixth grade students every year, because each year the current sixth grade class would have received more rounds of treatment over the course of elementary school than the previous year. SCI did not complete this plan, but Dr. Koukounari included the data from the sixth grade students in the baseline data. Dr. Styles did not include this data." GiveWell's non-verbatim summary of a conversation with Giuseppina Ortu on June 20, 2014. Both studies include a similar number of participants at the first follow up: "At baseline (2008) there were recruited 5700 children while the follow-up rate one year later was 53.42 % (3045/5700)." Koukounari 2011, Pg 16; Styles 2011 Pg 13, Table 8 shows about 3030 students were included in the first year follow-up analysis.
- Pilot study: Styles 2011 and Koukounari 2011 have strengths and weaknesses in defining the sample for the pilot study. Styles 2011 includes a much larger number of individuals (Styles 2011, Pg 3, Figure 1b compared to 710 in Koukounari 2011, Pg 7, Figure 2). However, it is unclear whether the individuals in the follow-up were all in the original cohort or whether some were added to the sample later. The two reports indicate different numbers of students included in the study and retraced at each followup. We have seen two explanations for the differences:
- 80
"The baseline impact survey was carried out in March 2012 with the 1st follow (FU1) up being done in March 2014 prior to the mass drug administration in April 2014. This report summarises and discusses the results from the 2nd follow-up survey (FU2) which was carried out in the 22 sentinel schools in the districts of Balaka,Blantyre, Chiradzulu, Lilongwe, Mwanza, N. and S. Mzimba, Neno, Ntcheu and Ntchisi in March 2015." SCI Malawi impact study – second follow up, Pg 3.
- 81
- 82
- 83
SCI M&E timeline (May 2015). Reports with first follow up results expected:
- Côte d'Ivoire: Not specified. Data collection expected in either May or November 2015.
- Liberia: Delayed. New data not specified. Fiona Fleming, email to GiveWell, September 18, 2015.
- Ethiopia: Not specified. Data collection expected in September 2015.
- DRC: Not specified. Data collection expected in October 2015.
- Mozambique: Low quality data collected so far. Next round of data collection expected to provide more information. LSTM Mozambique trip report (May 2015).
- Tanzania: Was expected in September 2015. No recent update.
- Zambia: Not specified. Data collection expected in July 2015.
- Uganda: Not specified. Data collection expected in October 2015.
- Niger: SCI notes that data was collected in 2011, 2012, 2013, and 2014. Report was expected in September 2015. No recent update.
- 84
- Niger: “Praziquantel (using dose-pole corresponding to 40 mg/kg) and Albendazole (400 mg) were given to the target population regardless of infection status, during the mass drug administration campaign that took place 3–4 weeks after the surveys were conducted.” Tohon et al. 2008, Pg 3. “A total of 89% of the initial sample group were re-examined one year after baseline data collection and the first round of treatment with praziquantel and albendazole.” Tohon et al. 2008, Pg 4.
- Burundi pilot: “At baseline (2007) there were recruited 3616 children. At 2008 the 1st follow-up took place where 1188 children were retraced since baseline (i.e. follow-up rate=32.85 %). At 2nd follow-up (2009) there were 1004 children successfully followed up since baseline (i.e. follow-up rate=27.77%). Finally at 3rd follow-up (2010) there were 713 children successfully followed-up (i.e. follow-up rate=19.71%). Longitudinal analyses for the 4 years are presented in the next pages for these 713 children.” Koukounari 2011, Pg 6.
- Burundi other schools: “At baseline (2008) there were recruited 5700 children while the follow-up rate one year later was 53.42% (3045/5700).” Koukounari 2011, Pg 15.
- Malawi: “A longitudinal survey design requires baseline data collection from schools prior to the initiation of large-scale distribution of praziquantel and albendazole or mebendazole through the school-based platform. Follow up surveys will be conducted immediately prior to subsequent rounds of treatment for the life of the programme to monitor the impact of the health intervention.” SCI Malawi panel study, Pg 3. “During the baseline survey, cohorts of 125 children from Standards 1, 2 and 3 (aged approximately 6, 7 and 8 years) were randomly selected in each of the schools and enrolled into the study. [...] This group of selected children, now in standards 2, 3, and 4, as well as a new group of 40 Standard 1 children, were re-tested to measure the same indicators during the 1st follow-up.” SCI Malawi panel study, Pg 4.
- For all three studies, the methodology does not discuss a control group, and with context, it is sufficiently clear that there was not one.
- 85
"This survey year saw a switch from a longitudinal survey design to a cross-sectional design which occurred following internal SCI reviews of the data and issues arriving from field surveys. The change in survey design led to the ages of children included in the study to be altered slightly to allow for like for like comparison over time and to capture those with the highest burden of infection." SCI Malawi impact study – second follow up, Pg 3.
- 86
SCI notes that because children in a control group would be tested for infection, ethical guidelines would require that those found to be infected receive treatment and thus would no longer serve as controls.
- 87
Sources for the data in the tables:
- Niger: Tohon et al. 2008. SCI recently sent us a more recent study on the Niger program, SCI Niger panel study 2011. However, for reasons described elsewhere in this report, we continue to rely on Tohon et al. 2008.
- Uganda: Kabatereine et al. 2007.
- Burundi: Styles 2011, and Koukounari 2011. As we discuss elsewhere in this report, both analyses have methodological limitations, and it is not clear which is more reliable. The results are very similar for worm prevalence, and Styles 2011 reports an additional year of data, so we rely on the Styles 2011 data for worm prevalence. Styles 2011 does not report infection intensity, so we rely on Koukounari 2011 for that data.
- Malawi: SCI Malawi impact study – second follow up, Pg 11, columns for 6-8 year olds only.
- 88“Before treatment, the overall prevalence of S. heamatobium infection was 75.4% of the 1,642 enrolled children...One year after a single-dose praziquantel treatment (administered using the WHO PZQ dose pole) co-administered with albendazole (400 mg single dose) for deworming, the prevalence of S. haematobium infection was 38%.”
Tohon et al. 2008, Abstract. - 89
- "Before treatment...21.8% of children excreted more than 50 eggs/10 ml urine." Tohon et al. 2008, Abstract.
- "The overall prevalence of S. haematobium infection was 38% and 4.6% of children had heavy-intensity infections; only three (4.6%) among the latter excreted more than 500 eggs/10 ml." Tohon et al. 2008, pg. 4.
- 90"S. mansoni infection was observed only in 2 schools: Sabon Birni (3%) and Sanguile ́ (1.1%)." Tohon et al. 2008, Pg 3
- 91"Hookworm infection was observed in 3 schools; Sabon Birni, where the prevalence was 18.8 and in 2 other villages were the prevalence was 0.6%. Hookworm infection was not observed in the schoolchildren of the 5 other villages." Tohon et al. 2008, Pg 3
- 92Alan Fenwick, phone conversation with GiveWell, November 28, 2011.
- 93Styles 2011, Table 2 pg 2. The same means seem to be presented in Figure 1, Pg 3.
- 94Eggs per gram. All epg data are the average over all participants, including those not infected.
- 95Koukounari 2011, Figure 6, Pg 10.
- 96Styles 2011, Table 3, Pg 4.
- 97Koukounari 2011, Figure 6, Pg 10.
- 98Alan Fenwick, phone conversation with GiveWell, November 28, 2011.
- 99Styles 2011, Table 9, Pg 15.
- 100Koukounari 2011, Figure 21, pg 22.
- 101Styles 2011, Table 10, Pg 16.
- 102Koukounari 2011, Figure 21, pg 22.
- 103SCI Malawi impact study – second follow up, Table 3, Pg 11, columns for 6-8 year olds only.
- 104SCI Malawi impact study – second follow up, Table 3, Pg 11. The first follow up report stated that there were no heavy infections at baseline:
- SCI Malawi panel study, Pg. 11, Table 7.1.
- SCI Malawi panel study, Pgs. 19-20, Table 8.2, "Followed-up" column.
We don't know the reason for the change in results.
- 1052.2% at baseline to 0.0% at one year to 1.5% at two years. SCI Malawi impact study – second follow up, Table 3, Pg 11, columns for 6-8 year olds only.
- 1060.2% at baseline to 0.0% at both one and two years. SCI Malawi impact study – second follow up, Table 3, Pg 11, columns for 6-8 year olds only.
- 107SCI Malawi impact study – second follow up, Table 3, Pg 11, columns for 6-8 year olds only.
- 108SCI Malawi impact study – second follow up, Table 3, Pg 11 columns for 6-8 year olds only.
- 109
- Niger: "Very low prevalence (0.3 to 0.7%) of Ascaris lumbricoides infection was observed in 5 schools, while 3% of the schoolchildren were infected in 1 school (Sanguile) and no infection was observed in 2 schools (Kaou and Tabalak)." Tohon et al. 2008, Pg 3. “The very low prevalence of soil-transmitted helminth infection is in accordance with previous observations made in Niger [32] and in 2 other African countries, Mali and Chad [22,33], areas that are subjected to climatic conditions comparable to the most inhabited regions of Niger.” Tohon et al. 2008, Pg 5.
- Malawi: No Ascaris or Trichuris infection reported. SCI Malawi impact study – second follow up, Table 3, Pg 11, columns for 6-8 year olds only.
- 110
Results from Styles 2011. We report "as measured" results for Burundi; SCI also reports model results.
Baseline Year 1 Year 2 Year 3 Year 4 Ascaris in Burundi (pilot) 14.9% 12.9% 20.1% 10.6% 10.1% Trichuris in Burundi (pilot) 3.2% 1.8% 3.9% 1.5% 2.4% Ascaris in Burundi (other schools) 21.6% 11.7% - 9.1% - Trichuris in Burundi (other schools) 10.4% 10.0% - 4.3% - - 111
- Niger:
- "Eight villages located in schistosomiasis endemic regions were randomly selected to represent the two main transmission patterns in Niger: six villages located near permanent (Tabalak, Kokorou) or semi-permanent (Kaou, Mozague, Rouafi, and Sabon Birni) ponds and two (Saga Fondo, Sanguile) located along the Niger River. The villages represented the south-western region (Tillabe´ry) and the central-northern region (Tahoua) of the country, with four villages from each region. One village is located in the Sudanian climatic zone and the seven others are in the Sahelian climatic zone." Tohon et al. 2008, Pg 2.
- SCI told us that these locations "are not representative of the treatment population as a whole. They were selected to indicate the impact of treatment in schools with varying prevalence and intensity of both [types of schistosomiasis]." Anna Phillips, SCI Country Program Manager for Burkina Faso and Niger, email to GiveWell, October 13, 2011.
- Burundi pilot survey: “More precisely, the 12 schools were chosen based on 3 zones-believed at the time that they would have the majority of NTDs. 4 schools were selected randomly so that they represent the ‘STHs +Schisto +oncho’ zone (these were Musenyi, Nyamibu, Munyika, Rukinga); then another 4 schools were selected randomly so that they represent the ‘STHs +oncho’ zone (Mirombero, Kizuga, Ruzibira, Mudende) and finally 4 schools were selected randomly so that they represent STHs only endemic areas (Gatwe, Ruko, Condi, Gitobo). Such decisions were based on available historic data. Thus, SCI Programme Manager advised not to stratify the statistical analysis by province and so such results (i.e. stratification by province) are not presented anywhere in this report.” Koukounari 2011 Pg 6.
- Burundi other schools: it appears that schools were selected to be representative, though this is not fully clear in the reports we have seen.
- Styles 2011 says, "The selection of schools was done randomly from the non-pilot provinces; taking into account 11 separate ecological zones." Pg 13.
- Koukounari 2011 says, “At baseline (2008) there were recruited 5700 children while the follow-up rate one year later was 53.42% (3045/5700). For these set of studies as they were designed to cover almost all of the country, it is worthwhile to also examine stratifications of analyses by district and such results are also presented in the following subsections. However, in most of the districts the children were coming only from 1 school (see relevant graphs for district whenever n<200; when this is the case then this is only 1 school per district and thus results should be treated there with caution and programmatic decisions to be taken with reservations). Whenever/wherever this is the case, results should be interpreted with caution as just 1 school would be quite ‘risky’ to represent inference/decisions for a whole district.” Pg 16.
- Malawi: The schools seem to have been selected in a way that makes them representative of districts with moderate to high prevalence, which are those districts that receive annual treatment (low prevalence districts receive more limited treatment). The schools were selected only from districts found to have moderate schistosomiasis prevalence in SCI's mapping: "Method of sentinel site selection: SCI’s protocol is to monitor only in those districts where prevalence of schistosomiasis is moderate or high i.e. SCI does not monitor in non-endemic or low prevalence districts where a full control program is not implemented. All districts except Mzuzu City surveyed in the mapping in February 2012 were determined to have moderate prevalence of S. haematobium, and consequently all districts except Mzuzu City were included in the selection of sites to be monitored for this species (see Table 1). S. mansoni infection was more focal and only present at moderate prevalence in Chiradzulu, Blantrye Rural, Lilongwe City and Lilongwe Rural East. Following district stratification by S. mansoni infection, such that the number of schools selected for S. mansoni monitoring, reflected the frequency of moderate risk areas in the monitoring areas, 22 schools were selected that would be monitor S. haematobium infection with a subset of 9 schools which also monitor S. mansoni infection. Due to the low prevalence of STH’s, STH infection was only monitored in those schools where the Kato-Katz slides were already prepared for S. mansoni." SCI Malawi panel study, Pg 4; SCI's senior biostatistician told us that the sampling method would produce a sample representative of the treated districts. Michelle Clements, SCI Senior Biostatistician, conversation with GiveWell, October 15, 2014.
- Niger:
- 112
- Niger: "A total of 89% of the initial sample group were re-examined one year after baseline data collection and the first round of treatment with praziquantel and albendazole." Tohon et al. 2008, Pg 4.
- Burundi:Pilot schools: 33%: “Without taking into consideration the parasitological exams, at baseline (2007) there were recruited 3616 children. At 2008 the 1st follow-up took place where 1188 children were retraced since baseline (i.e. follow-up rate=32.85 %).” Koukounari 2011. 50%: Styles 2011 Pg 1, Table 1. Other schools: 53%: “At baseline (2008) there were recruited 5700 children while the follow-up rate one year later was 53.42 % (3045/5700).” Koukounari 2011, Pg 16. 80%: Styles 2011 Pg 14, Table 8. The discrepancy between the populations included in Koukounari 2011 and Styles 2011 is described in more detail below.
- Malawi: "Overall, the drop-out rate was higher than expected for both species of schistosomiasis. 48% of those pupils monitored for S. haematobium dropped out the study between baseline and follow-up, and 64% of those pupils monitored for S. mansoni dropped out of the study." SCI Malawi panel study, Pg 17. Since the most meaningful results from Malawi were for Schistosoma haemotobium, we focus on the follow-up rate for that species.
- 113
Benjamin Styles, SCI Senior Biostatistician, phone conversation with GiveWell, August 12, 2011.
- 114
"An initial analysis of approximately 2,000 individuals in selected sentinel sites has demonstrated an over 50% reduction in infection markers (both prevalence and intensity) following two rounds of treatment. Infection with either species of schistosomiasis has fallen from 19.8% at baseline to 8.3%, following two rounds of treatment, with less than 4% now harbouring heavy infections (and who are those most likely to develop severe morbidity)(Table 2)." Summary Technical Report: Schistosomiasis Control in Yemen (July 2014), Pg 4. Table with results for S. haematobium and S. mansoni is on Pg 5.
- 115
"As part of this, a cohort of 8,000 individuals (6,500 school-aged children and 1,500 adults) from 36 representative districts across the country were sampled for demographic and parasitological markers at baseline prior to intervention and following treatment. An initial analysis of approximately 2,000 individuals in selected sentinel sites has demonstrated an over 50% reduction in infection markers. [...] To confirm these results, and to determine whether they are reflected elsewhere, a full round of impact evaluation in all 36 districts will be implemented in September 2014 prior to the next treatment campaign." Summary Technical Report: Schistosomiasis Control in Yemen (July 2014), Pgs 4-5.
- 116
"At baseline in 2010, prior to the first treatment campaign, a small-scale mapping survey was carried out in in areas without previous mapping data. The results from these surveys (120 schools in 9 governorates) were combined with mapping surveys conducted from 2002-2010, along with ecological information relevant to schistosomiasis transmission obtained from the literature." Summary Technical Report: Schistosomiasis Control in Yemen (July 2014), Pg 3.
Results from "2010" include 333 districts, which seems to indicate that only a portion of this data (120 of 333 districts) was collected in 2010 and the remainder was collected several years before. Mapping of Schistosomiasis and Soil-transmitted helminths in Yemen, Pg 42. - 117
"After 2-3 rounds of treatment a prevalence re-mapping survey was conducted to map the distribution of infection and provide an overview of the programme’s impact on NTD prevalence from baseline levels in 2010, as well as set the control approach for upcoming years of the programme." Mapping of Schistosomiasis and Soil-transmitted helminths in Yemen, Pg 9. Full results on Pg 42, Table 13.
- 118
Citations for all statements in this list can be found in this spreadsheet, Methods sheet, see comments.
- 119
SCI told us, "Shehias were stratified by MoH treatment programme and by elimination programme; required sample size selected from each startum." Fiona Fleming, email to GiveWell, November 5, 2015. We don't know how to interpret this.
- 120
"In other areas the survey was easier but in Chinde Islands where Dr Xose went from one island to the next to find the selected village and got lost for a few days because the district has been divided into two and we had to select again the villages." Fiona Fleming, email to GiveWell, November 5, 2015 (quoting from email from FPSU, which runs the program in Mozambique).
- 121
Fiona Fleming, email to GiveWell, November 5, 2015 (quoting from email from FPSU, which runs the program in Mozambique).
- 122
Fiona Fleming, email to GiveWell, November 5, 2015.
- 123
- For Côte d'Ivoire, coverage reported by parents was lower than coverage reported by children. In Malawi, coverage reported by parents was similar to coverage reported by children. In Côte d'Ivoire, parents' answers were excluded from the reported results: "Calculation of validated coverage rates initially included answers from both proxy and direct interviews across all 4 districts. As shown in Figure 2, coverage rates calculated based on direct interviews were higher than those which included responses given by proxy (p < 0.001), perhaps due to the parent erring on the side of caution when giving their answer. As direct interviews are believed to be more robust, we omitted data from proxy interviews when calculating final coverage rates (Table 4)." SCI Côte d'Ivoire coverage survey 2014, Pg 10.
- In Malawi, parents' answers were included in reported results. Proxy results were similar to results from direct interviewing in Malawi, and were included in the headline analysis. SCI Malawi coverage survey 2012, Pg 11, Figure 4.
- About 9% of the responses in Côte d'Ivoire were from parents. SCI Côte d'Ivoire coverage survey 2014, Pg 9, Table 3.
- Number of yes/no answers obtained in person (summed across four districts): 2178
- Number of proxy yes/no answers obtained (summed across four districts): 228
- 124
Fiona Fleming, email to GiveWell, November 5, 2015.
- 125
- Côte d'Ivoire: “The surveyors may ask additional questions to remind the children and see if the answers seem believable, for example:
- Show children the dose poll and ask if the children remember it
- Ask the children what they remember about the pills (it is normal to remember praziquantel's bitter taste, size and smell)
- Ask the children how many pills they took (while trying to judge how many they should have received by getting them to stand near the dose pole)."
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014.
- For Malawi (2014), SCI told use that verification methods were used, but the data was not included in the survey report. Fiona Fleming, email to GiveWell, November 5, 2015.
- For Uganda, Zanzibar, and Zambia, SCI told us that the survey "asked if [respondents] recognised pills / dummy pills and dose poles'." Fiona Fleming, email to GiveWell, November 5, 2015.
- Côte d'Ivoire: “The surveyors may ask additional questions to remind the children and see if the answers seem believable, for example:
- 126
"The surveyors only record if the children say they took the drug, didn’t take the drug, or are unsure; currently, the surveyors do not track answers or concerns from the additional questions, though going forward SCI will consider including these as well." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014
- 127
"The actual sample included caretakers of 578 children." SCI Mozambique coverage survey 2015, Pg 5. Note that we have only received permission to publish a summary of this report. Quotation is from the full, unpublished report.
- 128
SCI Mozambique coverage survey 2015, Pg 23. Note that we have only received permission to publish a summary of this report. Quotation is from the full, unpublished report.
- 129
SCI Mozambique coverage survey 2015, Pg 24. Note that we have only received permission to publish a summary of this report. Quotation is from the full, unpublished report.
- 130
"Pole doses were used as a proxy for the medication – rather than showing the medication we showed them the poles. Only parents (not teachers) can authorize medication to kids in Mozambique and they need to be involved and informed during the social mobilization which is conducted usually by the district officers and the activists, in the week preceding the distribution of the medication. The activists use posters and poles when they inform the community and the poles are very recognizable. The poles are also used in the integrated campaigns – and in most of these districts campaigns have been conducted for a number of years. So…they may be recognized as part of a preventive medication campaign rather than related to the PZQ only." Fiona Fleming, conversation with GiveWell, November 5, 2015 quoting from an email from FPSU.
- 131
GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014
- 132
See notes in the "data quality control" column of this spreadsheet, sheet Methods.
- 133
Email from SCI's partner FPSU, quoted to us by SCI:
"Further to our conversation, here is a recount of the supervision of the survey:- Initially there were 6 teams with Cabo Delgado and Nampula divided into two. All of them were supervised by Don and myself during 2 days of intense data collection in Nampula Cidade to ensure the areas selected were visited, the random selection of houses and respondent and the correct administration of the questionnaire plus the team organization and supervision.
- Teams were then reduced to 4 as it made more sense to complete districts before traveling to the next.
- Each team had one or two supervisors, one being the provincial NTD or M&E staff in the case of Zambezia, the national supervisor being NTD or other MISAU Departments (Cabo Delgado, Zambezia). The district officers worked in teams so that most of the interviews in one district were done by the other district officers with no connection with the district. In fact in most cases the district officer of that particular district was solving logistical and administrative issues which are quite intense in Mozambique (permission by the provincial delegate, permission by the district and the locality chief letters of introduction all signed and stamped, motorcycles rental and bills etc).
- Nampula was identified as the most complex area and the team was supervised by me during the completion of Ilha and Mossuril districts plus Cidade Nampula while Don supervised District Nampula and again the finalization of Cidade Nampula which was pretty complicated. In other areas the survey was easier but in Chinde Islands where Dr Xose went from one island to the next to find the selected village and got lost for a few days because the district has been divided into two and we had to select again the villages. All other supervisors provided daily reports to Don. They also wrote a report of the questionnaires received every day, reviewed and sent.
- In most cases, data was sent to the database and reviewed every day. Once the supervisor had sent the questionnaire editing was only allowed to Don Whitson. Some areas did paper based questionnaires and this was again submitted and reviewed."
Fiona Fleming, email to GiveWell, November 5, 2015.
- 134
"MDA of PZQ across the 30 ICOSA districts were supported by the two partner organisations, SCI (ICOSA programme) and RTI (ENVISION programme), responsible for supporting SCH treatment in the country. ICOSA supported delivery in80 sub-counties and ENVISION in 47. Since the drug delivery may vary between the programmes, and thus potentially affect coverage, it was decided that stratification would be by the partner programme who supported the delivery of the MDA by the MoH i.e. ICOSA and ENVISION." SCI Uganda coverage survey 2014, Pg 6.
- 135
"We found significant differences between districts in validated coverage rates, with three out of the four districts surveyed having an overall validated coverage rate above the target of 75% set by the WHO." SCI Côte d'Ivoire coverage survey 2014, Pg 3.
- 136
- 137
LSTM Mozambique trip report (May 2015)
- "With authorization of Dra Olga, I am sharing with you the EXCEL file with results (not the databases), and she reminds me that the data belongs to MISAU." Pg 2.
- "The Team reviewed the results for 2012-2013-2014 and they confirmed that only 2 sentinel sites were strictly comparable for 2013-2014 (Mecula and Mandiba) and none of the Sentinel Sites for 2015 are going to be comparable to 2014. They decided to review the location of the new sentinel sites, to be able to have a better and stronger comparisons." Pg 2.
- 138
"The research summarised in this paper is based upon field-work funded by the Schistosomiasis Control Initiative (SCI), Imperial College, under the auspices of the Bill and Melinda Gates Foundation. [...] We are grateful to Professor Alan Fenwick, director of SCI, for his unfailing support, and his encouragement of our work, even when our findings made uncomfortable reading. We are also grateful to other staff from SCI, some of whom have disagreed with our analysis, but who have continued to provide assistance, including Lynsey Blair, Fiona Fleming and Artemis Koukounari." Allen and Parker 2011, Pg 114.
- 139
We examined the references from Parker, Allen, and Hastings 2007, Allen and Parker 2011, Parker and Allen 2011, Allen and Parker 2012, and Parker and Allen 2014, Muhumuza et al. 2013 and Standley et al. 2009. We searched on Google Scholar for "niger schistosomiasis prevalence," “niger deworming uptake," "niger praziquantel uptake," "Burundi schistosomiasis prevalence," "Burundi deworming uptake," "Burundi praziquantel uptake," "schistosomiasis prevalence Africa," "deworming uptake Africa," "praziquantel coverage Africa," "Uganda schistosomiasis prevalence," and "Uganda praziquantel uptake."
- 140
For example:
- SCI Director Alan Fenwick and SCI-affiliated researcher Narcis Kabatereine were coauthors on Brooker et al. 2005 and Standley et al. 2010.
- Narcis Kabatereine, SCI Africa Capacity Building Adviser, was a co-author on Standley et al. 2009.
- Lynsey Blair, SCI Senior Project Manager, was a coauthor on Stothard et al. 2013.
- Knopp et al. 2009 was funded in part by SCI: "Financial support: This study received funding from the Swiss National Science Foundation (projects PPOOB–102883 and PPOOB– 119129), the Natural History Museum (supported through The Health Foundation,United Kingdom),the World Health Organization (OD/TS- 07-00331), the European Union (FP6 STREP CONTRAST project, contract 032203), and the Schistosomiasis Control Initiative." Pg 1077.
- 141
See the spreadsheet for details and citations.
- 142
- 143
"The study was designed specifically to target schools on an ad hoc basis as an 'ambush' strategy, to prevent visiting only schools which are commonly surveyed or well-known by local health officers. By doing so, some of the more overlooked schools may have been sampled here, which correspondingly had lower incidences of treatment, irrespective of their prevalence levels." Standley et al. 2009, Pg 50.
- 144
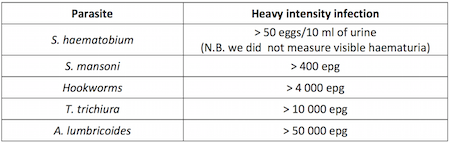
SCI Côte d'Ivoire panel study baseline report, Pg 7. - 145
"Single-dose oral therapies can kill the worms, reducing ... infections by 99 percent ... Reinfection is rapid, however, with worm burden often returning to eighty percent or more of its original level within a year ... and hence geohelminth drugs must be taken every six months and schistosomiasis drugs must be taken annually." Miguel and Kremer 2004, Pg 161.
- 146
GiveWell's notes from visit to Malawi on October 17-19, 2011. Updated in Alan Fenwick, SCI Director, email to GiveWell, November 24, 2014.
- 147
GiveWell's notes from visit to Malawi on October 17-19, 2011.
- 148
- Uganda: "The first country to implement a control programme on a national scale...Uganda implemented the SCI-supported control programme in April 2003." Kabatereine et al. 2007, Pg 91.
- Burkina Faso: "Some small-scale control activities with treatment had taken place in some areas in the past,11,13 but the national control programme did not start until 2004." Touré et al. 2008, Pg 780.
- Niger: "Niger’s National Schistosomiasis and Soil-Transmitted Control Programme (PNLBG) was launched at 2004." Fenwick et al. 2009, Pg 5.
- Mali: "In the following years many planned activities were not implemented due to limited financial resources but finally in 2004 national control activities recommenced in the country with support from the SCI." Fenwick et al. 2009, Pg 5.
- Tanzania: "The failure to embrace a national treatment programme has been due primarily to the costs involved in reaching the millions of individuals estimated to be at risk of infection, and the Ministry of Health was never able to support treatment within their budget. In October 2003, the Tanzanian National Plan was approved for funding by the SCI as a step towards developing a sustainable control programme." Kabatereine et al. 2006, Pg 334.
- Zambia: "'The Zambian Bilharzia Control Programme' (ZBCP) was established in 2004 to develop a MoH and MoE joint strategy for bilharzia and worm control. The MoE was already in receipt of a grant from the United States Agency for International Development (USAID) for implementing training and treatment in some schools on a small scale in two provinces, Eastern and Southern, which was known as the ‘School Health and Nutrition programme’ (SHN)." Fenwick et al. 2009, Pg 4.
- 149
"Without SCI's involvement, the program would likely not have gone forward. With the exception of filling small funding gaps on an ad hoc basis, the government has not been able to allocate funding to NTDs. It was interested in doing disease mapping but did not have the funding to do so, and it likely would not have received drug donations without the mapping data." GiveWell's non-verbatim summary of a conversation with Oumer Shafi, November 4, 2014.
- 150
"Drug distribution channels:
- School-based delivery for school children. School teachers will be trained to carry out drug distribution at schools.
- Community-based delivery for school-aged children who are not attending school and for community adults at high risk. Community Drug Distributors (CDD) will be trained to deliver the drugs at community.
- Health centre-based delivery. Drugs will be made available at health centres for those in the community who do not qualify for MDA and who request for treatment. Health workers at the centres will be trained.
Drug distributors need a minimum of one day’s training to understand the basis for calculating dosages, the necessary actions to deal with side-effects and treatment record keeping and reporting." SCI Neglected tropical diseases in Mozambique, Pg 23.
"For schistosomiasis and STHs, treatment will be conducted through schools by the teachers. For LF, treatment will be conducted through community directed treatment, by the CDDs and community health agents, managed by the district medical officer." SCI Proposal by SCI, Imperial College to manage the Program for Integrated Control of Neglected Tropical Diseases in Côte d'Ivoire, Pg 23. - 151
- "In Tanzania matters came to a head in places around Morogoro in 2008. Distribution in schools of tablets for schistosomiasis and soil-transmitted helminths provoked riots, which had to be contained by armed police. It became a significant national incident, and one of the consequences has been the delay in Tanzania adopting a fully integrated NTD programme, and the scaling back some existing drug distributions." Allen and Parker 2011, Pg 109.
- "From these reports a number of problems with the MDA were raised which included fear of side effects from the tablets, particularly following the mass hysteria and death in Blantyre and Rumphi respectively and may explain some of the geographic heterogeneity seen. Furthermore most districts reported that MDA occurred after standard 8 students had finished exams and left school, and due to having inadequate resources for drug distribution...The side-effects incident in Blantyre and death in Rumphi had a large effect on districts and with many district reports stating that after the incidence many families refused to participate." SCI Malawi coverage survey 2012 Pgs 5, 21.
- 152
Fiona Fleming, conversation with GiveWell, November 5, 2015.
- 153
Alan Fenwick, SCI Director, email to GiveWell, November 24, 2014.
- 154
SCI planned SCH treatment numbers by country by year (October 2015)
- $0.30 comes from the "0.25 cents per treatment" plus an additional 20% for "Central cost required (normally 20%)" since these assumptions are applied to most programs from April 2016 through December 2019.
- One exception is for Nigeria, where SCI estimates $0.40 per treatment and an annual central cost of $300,000 (roughly $0.50 per treatment from April 2016 - December 2019).
- For comparison, our estimate of SCI's cost per treatment, excluding drugs and in-kind government contributions, based on SCI's recent programs, is $0.53 per treatment (a portion of our total estimate of $1.26, with the remainder accounting for drug costs and government contributions).
- 155
- Fiona Fleming, SCI Senior Monitoring & Evaluation Manager, conversation with GiveWell, September 21, 2015.
- SCI's first Value for Money Officer left in May 2015, after only 6 months in the role. It hired a new Value for Money Officer, who was expected to join SCI in October 2015. Fiona Fleming, SCI Senior Monitoring & Evaluation Manager, conversation with GiveWell, September 21, 2015.
- 156
This is the period for which we have the most recent, and therefore we believe, the most accurate, data. Based on the history of these programs and the older data we've seen, we'd guess that there were fairly small costs for the Ethiopia and DRC prior to April 2013. GiveWell summary of SCI finances (October 2014), Sheet Combined with previous updates, and Alan Fenwick, email to GiveWell, September 28, 2015.
- 157
This understanding is from undocumented conversations with SCI from early in our investigation of SCI.
- 158
- "Ordering of ALB is carried out by the Ministry Of Health Programme Manager for Lymphatic Filariasis (LF) Elimination. Previously the ALB had been used for the LF program and stocks had not been replenished in time for the SCH campaign which contributed to the low ALB coverage. Treatments were also carried out in conjunction with the child health days which may have caused confusion with who was eligible for treatment and prioritising the younger children. Furthermore due to the complexities of distributing PZQ compared to ALB there may have been more focus during the training and distribution on reporting and dispensing PZQ." SCI Malawi coverage survey 2012, Pgs 20-21.
- "Miscommunication between the national Program Managers for lymphatic filariasis and schistosomiasis led many districts to believe that the ALB which they received should have been made available for the MDA but was not used." SCI Malawi coverage survey 2014, Pg 37.
- "Unlike in Sub-Saharan Africa, where SCI distributes praziquantel for schistosomiasis and albendazole for STH in equal amounts, Sudan has many areas where schistosomiasis is a problem but STH are not, and SCI distributes more praziquantel than albendazole. However, a small number of areas including Kassala and eastern Sennar have STH and no schistosomiasis. In these areas, the Ministry distributes more albendazole than praziquantel." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
- "Albendazole (ALB) was also distributed in some of the 30 districts under different partners, however ICOSA programme did not support its procurement, distribution or data collection in 2013/2014." SCI Uganda coverage survey 2014, Pg 4.
- 159
We explain why we take this approach in this blog post.
- 160
Alan Fenwick, SCI Director, email to GiveWell, November 24, 2014
- 161
It is not clear to us how to interpret the 87.4 million “treatments for all NTDs” in this data (e.g. how many of these were deworming and if SCI paid for the treatments), so to be conservative we have not included them at all. A more optimistic way to interpret these data could be to include 24.2 million schistosomiasis treatments in Burkina Faso, Niger, and Uganda that were delivered as part of integrated treatment programs (SCI Gates Foundation final report (January 2011), Pg 9, Table 2; these countries account for 70 million of the 87.4 million “treatments for all NTDs”). Including these 24 million additional treatments lowers the estimate to $1.17 per treatment.
- 162
See this spreadsheet for details. Note that this is not an ideal comparison because reported coverage rates are calculated from reported treatment numbers and an assumed target population. We would like to adjust the reported treatment numbers, rather than the reported coverage rate, but don't have the data to do so. It is possible that the difference in the reported coverage rate and the coverage rate from the coverage surveys is due to errors in the numbers used for the target population rather than the reported treatment numbers.
- 163
We used Leslie et al. 2011, a study of the costs of a SCI-funded deworming program in four districts of Niger in 2004-2006, to estimate non-SCI contributions to SCI's deworming programs. Three of the authors of the study were affiliated with SCI. The study aimed to account for all costs of the program, including costs funded by the government and non-financial costs such as the value of volunteers' time:
“This was a retrospective study which covered a two year period from April 2004 to May 2006, including the first and second years of MDA and related programme activities in four health districts. All data on first year costs at national, regional, district, and sub district levels were taken from the PNLBG accounts and receipts and records of staff missions or activities. Second year cost data for national and regional level activities were taken from receipts. District and sub district, school and community MDA resource use data for 2005 were collected in June 2006 through a retrospective survey…
The main cost elements include: the programme specific expenditure; the opportunity cost or value of government contributions related to in-kind costs of using local government staff and vehicles and the value of CDD’s time (taken as the daily agricultural labour rate); and the international costs of programme co-ordination, reporting and technical support." Leslie et al. 2011, Pgs 23.The study is of a single country, looked at a program that was carried out years ago, and the program may differ in some ways from current programs, but overall it is of high quality and provides us with a sense for the portion of resources contributed by SCI versus non-SCI parties.
Two examples of how the area where the study was conducted may not be representative of all areas in which SCI works:
- Due to low school enrollment rates, a substantial portion of the program was through community distribution. Current SCI programs focus on school-based distribution. "The primary school net enrolment rate (NER) in 2004 in Niger was 41%... To achieve high treatment coverage in targeted school age children and at risk adults two treatment strategies, school-based and community-based distribution, were established." Leslie et al. 2011, Pg 2.
- "The cost per treatment and prevalence figures relate to the study sample of four districts located in the Niger River Valley. This was and is an area of high disease prevalence and high population density relative to other parts of the country. The costs per person treated may be higher in lower density and more remote areas." Leslie et al. 2011, Pg 8.
Non-SCI costs were 18% of the total cost of the program and 33% of the cost of school-based deworming (the program also included community-based deworming).
- ”Programme cost: 75%
- Government cost: 18%
- International tech. support: 7%”
Leslie et al. 2011, Pg 5, Table 2.
It is our understanding from the paper and our past conversations with SCI that "programme expenditure" was fully funded by SCI. We believe that "international tech. support" refers to SCI staff time and travel costs; we're somewhat less confident in this than in our understanding of “programme expenditure.” Government costs are "related to in-kind costs of using local government staff and vehicles and the value of CDD’s time (taken as the daily agricultural labour rate)." Leslie et al. 2011, Pg 3.
Calculating non-SCI costs of school-based delivery:
- The average cost/treatment in the study was $0.58: “The total economic cost per treatment was $0.58. This includes programme, government and international costs.” Leslie et al. 2011, Author Summary. At 7% of the total cost, international tech. support accounts for $0.04/treatment.
- “The full economic delivery cost of school based treatment in 2005/06 was $0.76, and community treatment was $0.46. If only programme costs are included these figures are $0.47 and $0.41 respectively.” Leslie et al. 2011, Pgs 7-8.
- Therefore, non-program costs (government and international tech. support) are $0.29 ($0.76 - $0.47) of the $0.76 cost of each school based treatment. Since $0.04 is international tech. support, that leaves $0.25 of government costs, or 33% of the total cost.
It is our understanding that in recent programs SCI has continued to do some community-based deworming but that most of its treatments are delivered through schools. Therefore, we conservatively estimate that non-SCI actors contribute 30% of the cost of a SCI deworming program.
- 164
"Imperial College pays the majority of SCI’s overhead costs, including rent and utilities, and offers free services such as legal assistance. Imperial’s legal department prepares all of SCI’s contracts. The college also covers some risks and liabilities that SCI may face. In return, SCI pays Imperial 6% of its funding from DFID, but this does not cover the full cost of the services that SCI receives. The 6% of the DFID funding that is paid to the college is not included in SCI’s budget, but is included in the total size of the DFID grant. SCI may perform an analysis of the costs covered by Imperial College, but this is not currently a high priority." GiveWell's non-verbatim summary of a conversation with Wendy Harrison and Najwa Al Abdallah on September 8, 2015, Pg 4.
- 165
“Program costs can vary. For example, in Sudan, it can be expensive to transport drugs. In Darfur, it might cost about 40-50 pence per treatment, while in Khartoum it could be 10 pence per treatment.” Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014.
- 166
Sources for this data:
- Bleakley 2007: Pg 84, Table 1, "Hookworm-Infection Rate," "Whole Sample."
- Croke 2014: Kabatereine et al. 2001, Pg 284, Table 1, Average for eastern districts. Kabatereine et al. 2001 was a disease mapping study conducted in southern Uganda in 1998, two years before the study underlying Croke 2014 began, I.e. these are not results from the individuals enrolled in the study underlying Croke 2014. Note that the districts in the eastern district average in Kabatereine et al. 2001 are not an exact match for the districts included in Croke 2014, though four of the five districts included in Croke 2014 (Busia, Iganga, Mbale, and Tororo) are included in the Eastern district average. Furthermore, the districts for Croke 2014 were selected because Kabatereine et al. 2001 had found high worm prevalence in eastern districts: "Five districts in the eastern region of Uganda were selected (Busia, Iganga, Mbale, Palissa, and Tororo) because a survey had indicated that about 60% of children aged 5-10 years were infected with intestinal nematodes, most commonly hookworm." Alderman et al. 2006, pg 1.
- Miguel and Kremer 2004: Miguel and Kremer 2004, Pg 168, Table 2.
- Summary of SCI data from previous programs: Based on our discussion of the Niger, Burundi, Burkina Faso, and Uganda panel studies in our 2012 review of SCI.
- Liberia: SCI Liberia panel study baseline report, Pg 4, "Summary table of baseline results."
- Malawi: SCI Malawi panel study, Pg 11, Table 7.1.
- Côte d'Ivoire: SCI Côte d'Ivoire panel study baseline report, Pg 11, Table 6.1.1
- Zambia: SCI Zambia panel study baseline report, Pg 11, Table 7.
- Uganda: SCI Uganda panel study baseline report Pg 10, Table 6.1.
- Zanzibar: Knopp et al. 2013: "The baseline Schistosoma haematobium prevalence in school children and adults was 4.3% (range: 0-19.7%) and 2.7% (range: 0–26.5%) in Unguja, and 8.9% (range: 0–31.8%) and 5.5% (range: 0–23.4%) in Pemba, respectively. Heavy infections were detected in 15.1% and 35.6% of the positive school children in Unguja and Pemba, respectively." Abstract. This study also measured disease rates in adults and the treatment program will include adult treatments.
Bleakley 2007, Croke 2014, and Miguel and Kremer 2004, are discussed in greater detail here.
The WHO definition of "heavy" infection, which seems to have been used across all of the studies, is given in this table:
SCI Côte d'Ivoire panel study baseline report, Pg 7. - 167
- For schistosomiasis, mapping data was given in the form of number of districts with schistosomiasis prevalence ≥50%, ≥10% and <50%, and ≥1% and <10%. As an estimate, we assumed that these ranges correspond to average prevalences of the midpoint of the range: 75%, 30%, and 5.5%, respectively.
- For STH, mapping data was given in the form of number of districts with STH prevalence ≥50%, ≥20% and <50%, and ≥1% and <20%. As an estimate, we assumed that these ranges correspond to average prevalences of 75%, 35%, and 10.5%, respectively.
- We assumed that SCI would provide treatment in all areas, including low risk STH areas. The mapping report notes that WHO does not recommend MDA for STH in low risk areas (Pg 9), but it is our understanding that SCI generally treats for STH wherever it treats for schistosomiasis, which may include some districts at low risk for STH.
- We have assumed that no child has more than one STH and that prevalence of each STH is the same. This is unlikely to be accurate, but serves as a lower bound.
- 168
"In Malawi, urine volumes were not accurately recorded thus it is possible that data is indicating lower overall prevalence in sentinel sites. ICOSA will be undertaking further data analysis to quantify underestimates using mapping data from 2012 and baseline data in appropriate districts." SCI report to DFID (October 2013), Pg 15.
- 169
"The NTD programme in Zanzibar has recently completed the 3rd round of MDA." SCI report to DFID (October 2013), Pg 17.
- 170
See our page on money moved to top charities.
- 171
Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014.
- 172
Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014.
- 173
“In extreme circumstances, committed money could be shifted to other opportunities. For example, SCI had planned to do work in Liberia, but the Ebola outbreak has put that work on hold and so the committed funding could be reallocated.” Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014
- 174
- ”SCI first contacted the government [in Côte d'Ivoire] and started to discuss a SCH/STH program in 2010. A civil war delayed progress because there was political turmoil, a weakened health system, and dangerous conditions. In 2012 conditions improved, and the contracts between SCI and the Ministry of Health were set up.” GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014, Pg 1.
- ”Using drugs that are about to expire is a key factor used to prioritize between programs in strategic budget decisions.” Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014.
- “Factors that could affect SCI’s plans include country capacity (countries not being prepared to use planned funding or asking to expand more quickly than planned), WHO praziquantel donations (countries getting more or less drugs than expected), and new countries asking for assistance. New restricted funding could shift unrestricted funding to another use.” Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014.
- Treatment frequency is determined by mapping results: "World Health Organization (WHO) guidelines suggest different treatment frequencies depending on prevalence:
- Low (1-10% prevalence): treat twice during primary school (once every 3-4 years)
- Moderate (10-50% prevalence): treat every other year, and
- High (prevalence over 50%): treat every year.
Only 3 districts have high prevalence so the plan for next year is to treat those areas, as well as those that need treatment every other year and were not treated in 2014. Others districts have moderate or low prevalence and would be treated again in future years, following WHO guidelines." GiveWell's non-verbatim summary of a conversation with Sarah Nogaro, October 16, 2014, Pg 2.
- 175
- Comparing our conversations from 2013 to what happened in 2014 provides some context. In October 2014, SCI told us that if it had received an additional £1 million (about $1.6 million) at the beginning of 2014 it would have used the money to increase the size of each country's budget by 10-20%, which would have been used to make the programs more comfortable but would not have led to more treatments. Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014. (As of November 4, 2014, Google stated that £1 is worth $1.6.) In November 2013, SCI told us that it would likely use additional funding to fund two existing programs and to start two additional programs. Expectations as of November 2013 for how it would spend an additional $4 million:
- Côte d'Ivoire: expected to need $400,000 and actually spent about $350,000.
- Mozambique: expected to need as much as $3 million and actually spent $1.4 million.
- Mauritania: expected to need $1 million and didn’t spend anything.
- Ugandan islands: expected to need about $600,000 and didn’t spend anything.
- The $1.75 million spent in Côte d'Ivoire and Mozambique represents about 80% of the spending.
- Expectations as of 2013 are listed in our November 2013 review of SCI.
- Actual spending is through mid-September 2014 from GiveWell summary of SCI finances (October 2014).
- See also our discussion of budget revisions in 2015 in our August 2015 update on SCI.
- Comparing our conversations from 2013 to what happened in 2014 provides some context. In October 2014, SCI told us that if it had received an additional £1 million (about $1.6 million) at the beginning of 2014 it would have used the money to increase the size of each country's budget by 10-20%, which would have been used to make the programs more comfortable but would not have led to more treatments. Alan Fenwick, SCI Director, conversation with GiveWell, October 15, 2014. (As of November 4, 2014, Google stated that £1 is worth $1.6.) In November 2013, SCI told us that it would likely use additional funding to fund two existing programs and to start two additional programs. Expectations as of November 2013 for how it would spend an additional $4 million:
- 176
"Main Outcomes of Visit
- Received formal mapping report and protocol
- Meet with Nigerian partners and Sightsavers to discuss report, possibilities of collaborating with SCI and where we can offer support
- Determine gaps within the Nigerian program that SCI could fill."
- 177
GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, October 2, 2015.
- 178
"Two foundations have asked SCI to submit grant proposals. One grant would be for $500,000 to strengthen SCI’s programs in Malawi, and the other would be for £100,000 to strengthen SCI’s programs in Madagascar. The latter would reduce the budget deficit in Madagascar from £600,000 to £500,000." GiveWell's non-verbatim summary of a conversation with Alan Fenwick and Najwa Al Abdallah, September 14, 2015.
It previously received a $1 million grant over three years for its work in Madagascar. Alan Fenwick, email to GiveWell, October 15, 2015. - 179
A British fundraising organization and an oil company have both made moderate contributions (£100,000, or about $160,000, each) and could potentially contribute more.
- ”Comic Relief, an organization that raises nearly £100 million per year from the British public, has given £100,000. It has previously targeted HIV and malaria but is now considering NTDs.” Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014
- ”Vitol was interested in contributing to charitable causes in countries where it drills for oil. It provided £100,000 to support mapping in Côte d'Ivoire and has since shown some interest in providing funding for implementation.” Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014
- As of November 4, 2014, Google stated that £1 was worth $1.6.
In 2015, SCI told us about two additional potential funders. It seems unlikely that these funders will significantly reduce SCI's funding gap: "Two groups, Sustainable Health and Epic Foundation, have expressed interest in conducting evaluations of SCI. SCI is now on each group’s short list of 100 charities to investigate. Both Sustainable Health and Epic plan to eventually select 10–20 charities to recommend. Epic will then approach its donors in an attempt to raise a total of $1 million in a year, which will be divided among its 20 selected charities, for a total of about $50,000 to each charity." GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, July 31, 2015.
- 180
”Historically, SCI has spent very little time on traditional fundraising activities. SCI may consider hiring a staff member dedicated to fundraising. Also, Imperial College has expanded its fundraising team, and it may be able to support SCI’s efforts to raise funds.” Alan Fenwick, SCI Director, conversation with GiveWell, October 14, 2014.
SCI noted that it has not put resources toward fundraising in the past due to the significant funding it has raised due to GiveWell's recommendation. Alan Fenwick, email to GiveWell, October 15, 2015.
- 181
Alan Fenwick, email to GiveWell, October 15, 2015.
- 182
This is the amount tracked in our 2014 "metrics year": February 2014 to January 2015. See our page on money moved to top charities.
- 183
£4,716,590. SCI draft financial statements for 2013/14 and 2014/15. As of October 12, 2015, Google states that this is worth about $7,237,000.
- 184
SCI planned SCH treatment numbers by country by year (October 2015)
- 185
"This gap when we wrote in September did not account for any [funder name] funding, basically because at that time [funder name] had not finalised their agreement, and we were not certain until the contract was signed how much they would offer. Having said that I must now update you because Mike French tells me that for Ethiopia [funder name] have finally signed an agreement with the government and transferred the first years money ‐ $2 million. That therefore does indeed reduce the gap for all three years although the $2 million may not all be for what we would have spent money on so I hesitate to reduce our contribution by the full $2 million. We are expecting that [funder name] will disburse $2 million each year so that is good news. If we hit our fund raising target therefore we will have some extra flexibility and Mike has come back with some further needs because the programme in Ethiopia is hoping to target adults for treatment with schistosomiasis and of course the Merck praziquantel donation is only for treating children so he would like us to buy some if possible. (10 million tablets for $1 million). However we need to think this through, for all our countries and we have a meeting with DFID and WHO in the coming weeks because the praziquantel needs for adults is becoming a hot issue." Alan Fenwick, email to GiveWell, October 29, 2015.
- 186
Our summary of SCI's plans for April 2016 to March 2017 (original source: SCI planned SCH treatment numbers by country by year (October 2015)).
- 187
Our summary of SCI's plans for April 2016 to March 2017 (original source: SCI planned SCH treatment numbers by country by year (October 2015)).
- 188
GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, October 2, 2015.
- 189
SCI planned SCH treatment numbers by country by year (October 2015).
We don't know why the data for April 2018 to December 2019 isn't given on a budget year basis. - 190
SCI draft budget 2015-2016, which SCI sent to us in March 2015, notes that SCI expected to spend GBP 5,140,368 in unrestricted funds in April 2015 to March 2016. It also notes that SCI held GBP 4,188,193 in unrestricted funds as of March 2015. However, SCI draft financial statements for 2013/14 and 2014/15, which SCI sent to us in July 2015, notes GBP 5,232,150 as of March 2015. (We discuss this discrepancy in our August 2015 update on SCI.) If we assume the document we received later has the correct balance as of March 2015, then SCI expected to spend all but about GBP 92,000 of the unrestricted funds it held as of March 2015. Note that given lack of consistency in the figures we've seen and lack of a more recent update, we have low confidence in the accuracy of our understanding.
- 191
Rough calculation of SCI's unrestricted revenue since April 2015:
- In July 2015, GiveWell granted $333,414 to SCI, which included all donations received in February through May 2015.
- Between June and September 2015, GiveWell tracked about $610,000 to SCI as a result of GiveWell's recommendation, including about $177,000 to GiveWell for the support of SCI, and $435,000 that was given directly to SCI (primarily from two gifts for $333,000 and $100,000).
- SCI told us, "SCI is now receiving monthly contributions from 3,000 individual donors and feels confident that through these donations, it will be able to build reserves of at least £500,000 during Q2, Q3, and Q4 of 2015." GiveWell's non-verbatim summary of a conversation with Alan Fenwick, SCI Director, July 31, 2015. According to Google's currency converter on October 3, 2015, £500,000 was worth about $760,000.
The sum of above is $1.7 million.
- 192
This is based on internal data on how much SCI received due to GiveWell's recommendation between November 2014 and January 2015 (which are the months when a high proportion of gifts are given) and SCI's total for unrestricted revenue (SCI financial statement 2013/14 and 2014/15 (revised October 2015)).
- 193
"SCI will start building its reserve from 1 April 2016. The closing balance of unrestricted income at 31 March 2016 will not be designated 100%. GBP 436,000* will be allocated to the reserve. [...] *The figure is the average monthly expense of FY2014/2015." SCI draft reserves policy (September 2015). According to Google's currency converter on October 3, 2015, £436,000 was worth about $662,000.
- 194
WHO schistosomiasis treatment gap data.