Note: This page summarizes the rationale behind a GiveWell-recommended grant to PATH. PATH staff reviewed this page prior to publication.
In a nutshell
In March 2024, GiveWell recommended a three year, $18.2m grant to PATH to provide technical assistance (TA) to the governments of Burkina Faso, the Democratic Republic of the Congo (DRC), Mozambique, Nigeria and Uganda to support the nationwide rollouts of malaria vaccines.
GiveWell recommended this grant because:
- We think PATH's proposed TA activities will moderately accelerate vaccine rollout and increase the quality of the rollout in the five countries included in the grant.
- We think that a faster and higher quality vaccine rollout will lead to more children being vaccinated against malaria, which will prevent mortality and morbidity from malaria.
- We think there is an urgent funding gap for these activities that would not be filled in the absence of this grant.
Our main reservations about this grant are:
- We think the malaria vaccine rollout is likely to achieve fairly high coverage in these five countries even in the absence of this grant due to high existing stakeholder buy-in.
- We are uncertain about the exact TA activities PATH will conduct, which makes it difficult to estimate the specific impact that this grant will have.
- This grant may have a limited learning value, due to the lack of good comparators to estimate a counterfactual.
Published: January 2025
Table of Contents
1. Summary
1.1 What we think this grant will do
This grant will fund PATH to provide three years of technical assistance (TA) to support the malaria vaccine rollout in Burkina Faso, the Democratic Republic of the Congo (DRC), Mozambique, Nigeria and Uganda. PATH's TA will include supporting countries in planning for vaccine introduction, coordinating stakeholders, engaging communities to promote demand, and strengthening in-country data systems to improve monitoring and better respond to implementation challenges. (more)
1.2 Why we made this grant
We are fairly uncertain about the level of impact PATH's TA will have, but our best guess is that this grant will be at least 10 times as cost-effective as unconditional cash transfers (GiveWell’s benchmark for comparing different programs). We base this on a threshold analysis we conducted, in which we estimate that PATH's assistance only needs to have a modest positive effect on vaccination rates in order for this grant to meet our funding bar of 10x cash. (more)
In simple terms, we think this grant will be cost-effective because:
- We think PATH's proposed TA activities will moderately accelerate vaccine rollout and increase the quality of the rollout in the five countries included in the grant. This is because PATH's support is designed to overcome likely obstacles to effective implementation. (more)
- We think that this faster and higher quality vaccine rollout will lead to more children being vaccinated against malaria, which will prevent mortality and morbidity from malaria. (more)
- We think there is an urgent funding gap for these activities that would not be filled in the absence of this grant. (more)
You can see the threshold cost-effectiveness analysis for this grant here.
The other factors informing our decision to make this grant are:
- PATH has a strong track record of supporting vaccine rollout, and has experience with malaria vaccine implementation specifically. (more)
- We have a strong qualitative impression of PATH's team, and believe that they are well-positioned to take on this work. (more)
1.3 Main reservations
- We think the malaria vaccine rollout is likely to achieve fairly high coverage in these five countries even in the absence of this grant. This is because governments are placing a high priority on malaria vaccine rollout, there is likely strong demand for the vaccine among caretakers, and there are other TA providers working in some countries. (more)
- Our understanding is that much of PATH's TA activities will take place at the national level, while many of the most challenging obstacles to an effective rollout may occur at the subnational or community level. (more)
- We are uncertain about the exact TA activities PATH will conduct, which makes it difficult to estimate the specific impact that this grant will have. This is in part because PATH plans to tailor its assistance to needs that arise in each country during the vaccine rollout. (more)
- It's possible we will have a limited ability to learn from this grant. This is because we can't know what coverage rates would have been in the absence of this grant, and other countries are unlikely to serve as good comparators due to differing contexts and data quality concerns. Additionally, the expected effect size of PATH's work is quite small, which would make it difficult to measure even if we had accurate and comparable data. (more)
2. The organization
PATH is a global non-profit launched in 1977 which works in a number of health areas, including malaria, with the goal of promoting health equity.1 In January 2022, GiveWell recommended a grant to PATH to accelerate the rollout of the RTS,S malaria vaccine in Ghana, Kenya, and Malawi. The malaria vaccine was piloted in areas of these three countries through the Malaria Vaccine Implementation Programme (MVIP),2 and our 2022 grant to PATH was to speed up introduction of the vaccine in areas used as comparators during the pilot.
GiveWell coordinated with PATH’s Center for Vaccine Innovation and Access in our investigation of this grant.
3. Planned activities and budget
Malaria is a key driver of under-5 mortality in sub-Saharan Africa.3 Malaria vaccines attempt to stimulate an immune response against the parasites that cause malaria, thus averting morbidity and mortality from malaria. RTS,S/AS01 (RTS,S) and R21/Matrix-M (R21) are malaria vaccines delivered in a series of four doses beginning at five months of age or older, with three doses given at monthly intervals and the fourth dose 12 to 18 months after the third.4 These vaccines are relatively expensive compared to other vaccines (~$4 per dose of R21; ~$10 per dose of RTS,S).5 Both have been shown to effectively reduce symptomatic malaria cases caused by P. falciparum. Evidence from phase-3 clinical trials suggests that receiving three doses of the malaria vaccine has an efficacy against clinical malaria between 55% (RTS,S)6 to 75% (R21)7 during the first year after the primary series. Additional detail is available in our updated report on malaria vaccines, which is forthcoming.
Both vaccines have been recommended for malaria prevention by WHO,8 and as of November 2023, Gavi had approved applications to introduce either R21 or RTS,S in 18 countries.9 Gavi has also approved small amounts of funding for technical assistance to support the rollout of the vaccine in some countries, but our understanding is that this is insufficient to meet country introduction and technical assistance costs.10
We think technical assistance (TA) can help to address some challenges common to new vaccine introductions, and additional challenges unique to the malaria vaccine, including (but not limited to):
- A need for coordination between countries’ national malaria programs and national immunization programs, which haven’t had to work together on this scale before (more);
- The need to build community awareness and trust in a new vaccine, and the potential for misinformation to spread (more);
- An administration schedule for malaria vaccines that doesn’t line up with existing immunization touchpoints (more);
- The susceptibility of vaccine rollout to external shocks (e.g., weather, political events, other emerging health priorities), which may negatively impact implementation (more).
3.2 Activities we expect this grant to fund
With funding from this grant, PATH will implement a three-year TA program to address these and other issues in five countries introducing the malaria vaccine in 2024: Burkina Faso, DRC, Mozambique, Nigeria, and Uganda.11 The activities PATH will carry out are broad in scope and are intended to ensure that pre-introduction planning, initial rollout, and scaled-up vaccine delivery go smoothly in each country.
Technical assistance will be provided at the national level in each country, with subnational support where specific problems arise and more support seems needed.12 The scale and scope of TA activities will differ by country depending on implementation needs, but will likely entail:13
- Conducting three regional workshops to enable cross-country learning about best practices and experiences from the malaria vaccine pilot, and to share guidance on developing introduction plans, training tools, and scale-up strategies.
- Providing technical expertise to countries to identify scope, opportunities, and needs related to vaccine introduction and scale up. This includes updating timelines and budgets, strengthening coordination between various stakeholders (including national immunization and malaria programs), supporting countries in incorporating malaria vaccines into their overall malaria control strategies, and assisting with national and subnational assessments of programmatic readiness, including cold chain and vaccine management capacity.
- Developing plans for community engagement and demand generation, to help increase demand for the vaccine and mitigate the risk of vaccine hesitancy and misinformation.
- Strengthening in-country data systems to enable better diagnosis and response to issues that might arise and conducting post-introduction evaluations of vaccine delivery.14
- Identifying specific budget gaps in each country and providing supplemental funds where necessary.
3.3 Grant timeline
The activities described above will be broken out into three stages:15
- Stage 1a (Q1 2024 to Q1 2025) - Regional workshops to support country planning and cross-country learning.
- Stage 1b (Q1/Q2 2024 to Q4 2025) - Integrated planning and budgeting for target countries and preparation for vaccine introduction.
- Stage 2 (Q3 2024 to Q4 2026) - Ongoing TA to support accelerated scale-up, uptake, and integration of the malaria vaccine.
Burkina Faso began rolling out the vaccine in February 2024, and other countries are planning to begin introducing the vaccine over the course of 2024.16 We made a small bridge grant to PATH in January 2024 to provide initial support pending our full funding decision, which PATH allocated to regional workshop planning and to priority TA activities in Burkina Faso.17
3.4 Budget for grant activities
The total budget for this grant across the three year period 2024-2026 is about $18.2 million.18 According to a budget we received from PATH, this amount will be broken down roughly into the following categories:19
- Personnel/consultants (25%)
- Travel - (5%)
- Regional, national, and subnational support - (40%)
- Other direct costs - (10%)
- Overhead - (20%)
4. The case for the grant
4.1 Cost-effectiveness
We believe that PATH's support will lead to a moderate increase in the number of children who receive malaria vaccines. Even though we’re highly uncertain about how large those increases will be, we think it's likely that this grant will be at least ten times as cost-effective as unconditional cash transfers ("10x cash), GiveWell's benchmark for comparing the cost-effectiveness of different programs). Our current funding bar is 10x cash.20
Based on our conversations with PATH and other stakeholders, our understanding is that malaria vaccines are very likely to be introduced without this additional support (see below). This is because country governments appear to be placing high priority on these vaccines, and global supply is expected to grow to meet demand in high- and medium-transmission settings over the next few years.21 As a result, our best guess is that making this grant would lead to relatively smaller coverage increases than other TA programs that we've modeled.22
Because we are so uncertain about the magnitude of the coverage increases PATH's TA will lead to, we've modeled a threshold analysis to determine what coverage increases would be required for this grant to meet our funding bar of 10x cash. Based on this analysis, we estimate that a 1.8 percentage point average increase in vaccine coverage among the target population over the course of the grant period will yield a value of at least 10x cash.
You can see a sketch of our threshold analysis here, using Uganda as an example:
| What we are estimating | Threshold value (for 10x cost-effectiveness) |
|---|---|
| Total grant to PATH | $18,200,000 |
| Under-five mortality benefits | |
| Number of years during which the grant would lead to higher coverage than under the counterfactual | 3 |
| Threshold input: Average difference in coverage rates between intervention and counterfactual, for the program to meet GiveWell's funding threshold | 2.2% |
| Annual births in areas of medium-to-high malaria transmission | 1,743,457 |
| Total additional children vaccinated if we make the grant | 116,812 |
| Costs per child vaccinated, PATH | $23.37 |
| Estimated malaria-attributable mortality rate among 5-59-month olds | 0.37% |
| Average reduction in malaria mortality among children receiving three or four doses of a malaria vaccine | 31% |
| Numbers of years of protection from full vaccination schedule | 4 |
| Malaria deaths averted in people aged 5-59 months | 538 |
| Value assigned to averting a malaria-attributable death of a person under age 5 | 116 |
| Units of value generated via deaths averted in the treated population | 69,609 |
| Initial cost-effectiveness estimate (mortalities averted among people under age 5 only) | |
| Initial cost per life saved | $5,072 |
| Initial cost-effectiveness estimate | 6.8 |
| Adjustments for other benefits | |
| Adjustment to account for mortalities averted among people age 5 and older | 5% |
| Adjustment to account for developmental benefits (long-term income increases) | 44% |
| Percentage of program impact coming from different benefits | |
| Mortality reduction in the vaccinated population | 67% |
| Mortality reduction in the untreated population | 4% |
| Long-term income increases in the general population | 29% |
| Supplemental adjustments | |
| Adjustment for additional program benefits and downsides | 42% |
| Adjustment for grantee-level factors | -9% |
| Adjustment for leverage and funging | -24% |
| Final cost-effectiveness (multiples of cash transfers) | 10.0 |
| Final cost per life saved (see here) | $4,678 |
We think this grant is likely to increase the number of children vaccinated with RTS,S or R21 malaria vaccines in the five countries targeted by the grant by moderately accelerating vaccine rollout and increasing the quality of the rollout.
We’ve heard from multiple global and country-level stakeholders that there are barriers that can slow down vaccine rollout or lead to lower coverage rates, and our impression from those conversations is that TA to countries beginning early in the vaccine introduction process can help to address many of those barriers and make vaccine rollout generally go more smoothly. The specific barriers will differ across countries, and part of the value that we think PATH will provide is to identify and proactively address barriers as they come up.23 Given that, and the relatively small amount of funding that this grant represents per country per year (~$1m), we have not deeply interrogated what the exact barriers to higher vaccine coverage would be in each country and how PATH’s activities will address those barriers.
Some of the potential mechanisms for PATH's impact may include:
- Strengthening coordination between national malaria programs and national immunization programs. The malaria vaccine is unique in that it will require coordination between these two parts of national health systems that have not had to work closely together in the past.24 PATH has noted a lack of established systems for coordination across these programs,25 and while we did not investigate this in much detail, we have heard repeatedly from stakeholders that this issue could be a bottleneck to implementation.26 We think it’s likely that these two health systems may work together more efficiently in the presence of a coordinating actor that has experience working with both parties (see below), and that better coordination may lead to a higher-quality vaccine rollout.
- Developing a communications strategy and community awareness activities around the new vaccine. PATH and other stakeholders have identified communications and community sensitization work as necessary when introducing new vaccines. Stakeholders in Uganda we spoke with noted that misinformation is already spreading around the malaria vaccine,27 and stakeholders in Nigeria pointed to similar problems in Nigeria and Cameroon.28 PATH’s proposed TA seems to emphasize both proactive and reactive communications, sensitization, and community engagement. PATH plans to coordinate with national and subnational stakeholders through Advocacy, Communications, and Social Mobilization (ACSM) committees,29 and supra-nationally via three regional workshops, to devise communications, media monitoring, and community listening strategies.30 We think these activities may contribute to caretakers, health workers, and community leaders trusting the vaccine and being more resilient to misinformation.31
- Supporting planning and communications around vaccine schedules. The malaria vaccine is administered in four doses that don't align with existing routine vaccination touchpoints, adding complexity to the introduction.32 PATH and other stakeholders have indicated that overcoming this complexity will require specific communications efforts33 and planning support to optimize the schedule in each country.34
- Reducing the impact of potential external shocks. Vaccine rollouts may face exogenous shocks (e.g., weather, insecurity, political/electoral events, new emerging health priorities or outbreaks) that can affect implementation. PATH has told us that having an experienced technical assistance provider can dampen the negative impact of shocks like these on vaccine rollout and allow normal implementation to resume more quickly afterwards.35 We did not spend time trying to triangulate this, though we did hear from stakeholders in DRC that they see some of the value from this kind of TA as insulating the system from shocks,36 and we agree this is a plausible impact pathway.
- Assessing and planning for different vaccine administration methods. While the vaccine will initially be introduced on an age-based schedule in all five countries, stakeholders have pointed to the potential for non-age-based administration of the vaccine in the future (e.g., seasonal administration in settings where malaria is transmitted seasonally) and suggested that several countries may want to switch to this model.37 We think PATH’s assistance could make process changes like this happen more quickly, potentially leading to a faster switch to more impactful and context-specific delivery approaches.
- Helping to overcome inertia within ministries of health. Based on their experience in past vaccine introductions, PATH’s team has noted that MoHs are generally overburdened and face competing priorities.38 As an actor focused solely on malaria vaccines, PATH posits that it will add some value merely from ensuring that things are proceeding according to plan within ministries (e.g., meetings are happening, data are being shared, plans are being finalized and implemented, and challenges are being responded to). We did not interrogate this point specifically, but we did hear similar suggestions from other in-country stakeholders we spoke to as part of this investigation.39
Funding Gap
Our sense is that the TA activities PATH will carry out are under-funded and that we’re relatively unlikely to be crowding out other funding through this grant.40 Based on conversations we've had during this grant investigation, we don't think other potential funders are likely to put more funding into TA for malaria vaccine rollout in the short term.41 Because the proposed countries plan to start introducing malaria vaccines in 2024, the funding gap for these activities is time-sensitive.42 This urgency increases our confidence that other funding is unlikely to materialize in time to support those vaccine introductions.
4.2 PATH as an implementer
We think PATH is the right partner for this TA, based on their past experience working on vaccines and malaria programs generally, and on malaria vaccines programs specifically. Reasons for our strong impression of PATH as an implementer include:
- A strong track record supporting vaccine rollout. PATH was a key implementing partner in the large-scale pilot of malaria vaccine delivery in three countries (see our grant page here), which achieved high coverage of the third vaccine dose in a short period of time.43 PATH has also supported nationwide rollouts of other vaccines, including polio, HPV, rotavirus, and typhoid vaccines, in a similar capacity to how it plans to support malaria vaccines.44 Stakeholders we've spoken with have consistently said that PATH was uniquely well-positioned for this work.45
- Strong in-country relationships and experience. We've spoken with country experts who told us that PATH has strong working relationships within the ministries of health of the target countries, including with both national malaria and immunization programs, and that PATH is well-placed to coordinate between these actors.46 Intuitively, we think these relationships will allow PATH to improve the quality and speed of the vaccine rollout as a TA provider.
- Our strong qualitative impression of PATH's team. In our investigation for this grant, we had four calls and a day-long series of in-person meetings with PATH at its headquarters. In each interaction, we found PATH's team to be highly prepared and ready to answer both big-picture and granular questions with examples from their prior work. This makes us feel confident that PATH has a strong grasp of the challenges of vaccine delivery, is well-positioned to stay on top of fast-moving developments on malaria vaccines, and will be open and transparent with us in sharing information.
- Our experience with previous grants to PATH. We have previously recommended grants to PATH for implementing the RTS,S malaria vaccine in comparator areas of the MVIP pilot (see this page), conducting a perennial malaria chemoprevention (PMC) pilot in DRC (see this page), and conducting a PMC/RTS,S trial (see this page). These grants have gone broadly as expected so far.
5. Risks and reservations
We are highly uncertain about the impact PATH’s TA activities will have compared to the counterfactual, and it’s possible that impact could be quite limited. This is because:
- Malaria vaccine rollout would take place without this grant. We think the malaria vaccine rollout is likely to achieve fairly high coverage in these five countries even in the absence of this grant. Reasons for this positive counterfactual outlook include:
- High government priority. We've heard from PATH and many other stakeholders that country governments are particularly excited about the malaria vaccine.47 Intuitively, we think this bodes well for rollout, as there’s likely to be strong buy-in and relatively high priority placed on implementation, even without PATH’s support.48
- High caretaker demand. Malaria is already a known and feared disease among the parents of children who would be receiving the vaccine.49 As a result, we think there is likely less of a need for demand generation and community sensitization activities than there might be in other vaccine introductions.
- Multiple TA providers. PATH would not be the only TA provider in at least some of the countries covered by this grant.50 While PATH and other stakeholders suggested that this would allow the different providers to leverage complementary strengths,51 we think this makes the counterfactual a "some TA" rather than "no TA" scenario, and thus limits PATH’s added value over the counterfactual.
- PATH's TA will occur mainly at the national level. Many of the barriers to high vaccine coverage are likely to occur at the subnational and community/facility levels, while our understanding is that PATH's TA activities focus more on the national level, which could potentially limit impact. Several stakeholders noted that communications and engagement activities will especially depend on subnational contexts.52 While PATH will have staff working at subnational levels in DRC and Nigeria,53 and will work with local TA partners in Nigeria,54 our impression is that PATH’s activities for this grant, and its past experience, are centered on national-level TA.55 Because of this, we are more uncertain about the impact of this grant than we might be if PATH were proposing intensive activities at the community or health facility levels.
- We are uncertain about the exact TA activities PATH will conduct. We did not deeply interrogate the individual activities in PATH’s plan, and the exact activities to be carried out in each country can't be fully determined ahead of time, as PATH will tailor its assistance to needs that arise during the preparation and early implementation stages.56 This means that we don’t know the exact pathways to impact in each country. As such, during our investigation we sought to understand the barriers to implementation at a high level (see above), as well as to triangulate with third-party experts whether PATH’s plan seems likely to generate coverage increases and whether PATH is well-positioned for this work (see above). We feel fairly confident about each of these aspects, though we’re still highly uncertain about exactly how much impact the specific grant activities will have.
- We have a limited ability to learn from this grant. We think we’ll have limited ability to retrospectively learn about the impact of this grant, primarily because it will be difficult to know how well malaria vaccine rollout would have gone in the absence of this grant. There are a few reasons for this, including:
- We don’t expect to have good comparators. We've found that our TA grants are easiest to evaluate when we can compare the grant areas to similar areas that don’t receive TA, and when we have data from before TA begins. We think comparisons to other, non-PATH-supported countries will be very tenuous for this grant because context differs greatly across countries. We also won’t have data to show trends before TA begins, because in this case TA will be delivered alongside vaccine introduction.57
- Data quality concerns. We will be mainly relying on facility-reported data to estimate coverage in PATH's target countries, and while PATH’s plans do include some degree of data system strengthening (more), we remain unsure about the quality of this data.
- Small expected effect size. Even if we could get high quality coverage data, we think it would have limited value because the increase in coverage that we expect from this grant is fairly small (1.8pp increase over the counterfactual for the three years of this grant period for this grant to be 10x cash). It might be difficult to assess whether the grant had an impact of that size even with high quality coverage data in both the grant and comparator countries.
In addition to the concerns about direct impact listed above, we have several other uncertainties around this grant, including:
- Impact on other malaria interventions. Because the malaria vaccine is relatively more expensive than other malaria interventions, some stakeholders expressed concern that shifting funding towards vaccine procurement will divert resources away from cost-effective programs (such as insecticide-treated nets).58 Because organizations that fund malaria interventions often rely on the same donors, donor countries prioritizing the vaccine would likely cause the already large funding gap for non-vaccine malaria interventions to grow. While we agree that this poses a longer-term risk (which we need to explore further), these concerns seem less relevant for this specific grant because we are not directly contributing to vaccine procurement. Because the vaccine rollout will take place anyway, we think that it’s better for it to go well, which we believe PATH’s TA can contribute to. We note that one of the two stakeholders who voiced concern about the vaccine agreed that this type of involvement by GiveWell seems prudent.59 We also considered whether we should be concerned about vaccines diverting resources or attention from broader malaria control at the country level. Our conversations with stakeholders left us less concerned about this, as funding for core malaria interventions like nets and seasonal malaria chemoprevention is often designated for those programs and therefore not fungible.60
- Longer-term risk of crowding out funding. While we've judged the risk of short-term crowdout as low (more), it’s possible that this grant could be contributing to a longer-term crowdout by creating an expectation that external funding for vaccine implementation support will be available. We’ve heard in our stakeholder conversations that Gavi typically relies on other partners for implementation funding.61 We think there is a chance that by committing this funding, we’re helping to perpetuate this dynamic, though we put limited weight on this because several stakeholders indicated that significantly increased funding from Gavi for implementation support seems unlikely in any case.62
- Vaccine efficacy. We have a number of open questions around the efficacy of the malaria vaccine. Most experts we spoke to said the vaccine is effective and improves malaria control efforts more broadly,63
but two stakeholders suggested they’re not convinced by the evidence and feel the vaccine’s effectiveness is overstated.64
There are certain aspects of the vaccine for which we don’t yet have conclusive data, which could mean that we are overestimating the impact of the vaccine (and by extension, of this grant) on malaria incidence and mortality. Our questions about the vaccine include:
- How much is the effectiveness of RTS,S and R21 driven by the first three doses compared to the fourth dose?
- Should we be worried about potential rebound effects, i.e., higher malaria incidence compared to unvaccinated children once the protection wears off?
- What is the long-term efficacy of R21?
- We do not have the same high-quality data on the long-term effects of R21 as we have for RTS,S.
- How do we best model the interplay of ITNs, SMC and malaria vaccines?65
Additional detail on our key uncertainties will be available in our forthcoming updated report on malaria vaccines (our previous report is here).
6. Plans for follow up
- We plan to get vaccine coverage estimates and data quality audits from PATH as the vaccine rollout is implemented. As discussed above, coverage estimates might have limited value for assessing the grant's impact because we don't have a good counterfactual, but we think they will be generally indicative of how well vaccine rollout is proceeding. We plan to have follow-up calls with PATH to discuss whether it has enough information to identify data quality issues, and whether more intensive monitoring would be beneficial.
- Our assessment of how this grant went will be primarily qualitative. This assessment might involve reviewing PATH's post-introduction evaluations, doing a field visit to one of these countries to observe the program in action, and speaking with stakeholders and experts about how the vaccine rollout went. In addition, we may consider funding an independent qualitative evaluation of the rollout and how TA might have contributed to it.
- We plan to have regular conversations with PATH during the grant period to stay updated on its milestones and predicted timelines for each country. This will include more formal check-ins every 6 months to discuss progress, challenges, and learnings from each country.
7. Internal forecasts
| Confidence | Prediction | Date |
|---|---|---|
| 75% | All five countries will have introduced the vaccine by the end of 2024. | December 2024 |
| 85% | At least four of the five countries will have introduced the vaccine by the end of 2024. | December 2024 |
| 75% | We will have finalized an MEL framework together with PATH by June 2024. | June 2024 |
| 35% | We make another malaria vaccine-related grant to PATH by the end of 2025. | December 2025 |
| 35% | We make a malaria vaccine-related grant to a grantee other than PATH by the end of 2025. | December 2025 |
| 65% | We will have received 2025 coverage data from non-PATH-supported countries by July 2026. | December 2026 |
8. Our process
In investigating this grant, we relied primarily on conversations with PATH and with other expert stakeholders, including people in the countries targeted by this grant. The principal aim of these conversations was to triangulate our biggest open questions about this grant, namely whether PATH’s TA can be expected to lead to coverage increases and by what mechanisms. In all, we had five calls and one day of in-person meetings with the PATH malaria vaccine team. We also spoke with several international NGOs as well as stakeholders in Burkina Faso, Nigeria, Mozambique, Uganda, and DRC.
We also updated our report on malaria vaccines (our previous report is here and our update to this report is forthcoming) with new evidence from MVIP and vaccine trials, built a shallow CEA (forthcoming) and a threshold analysis, and reviewed PATH’s proposal slides for their TA activities.
9. Sources
{kind=link}
- 1
- "Launched in 1977 by three intrepid researchers, PATH was a new kind of health organization: a nonprofit that would deliver the expertise, resources, and innovations of private industry to improve health for all." PATH, "Who we are"
- "PATH’s global team of scientists, clinicians, designers, engineers, advocates, and experts from dozens of other specialties, all share the same goal: health equity. We partner with public institutions, businesses, grassroots groups, and investors to solve the world’s most pressing health challenges." PATH, "Who we are"
- PATH, "Malaria"
- 2
- “PATH is requesting funding to support the rollout of donated doses of the RTS,S vaccine in pilot areas of Ghana, Kenya, and Malawi that have not yet implemented the vaccine. Each of these countries has already implemented a pilot rollout of the vaccine.” GiveWell's non-verbatim summary of a conversation with PATH and WHO, January 5, 2022 (unpublished)
- “The MVIP is coordinated by WHO in close collaboration with ministries of health (MoH) in the three participating countries -Ghana, Kenya, Malawi -and a range of in-country and international partners. The MoH of the pilot countries have introduced the RTS,S/AS01 vaccine through their childhood immunization services using routine vaccine introduction strategies and methods.” WHO, Full Evidence Report on the RTS,S/AS01 Malaria Vaccine, 2021, p. 7
- 3
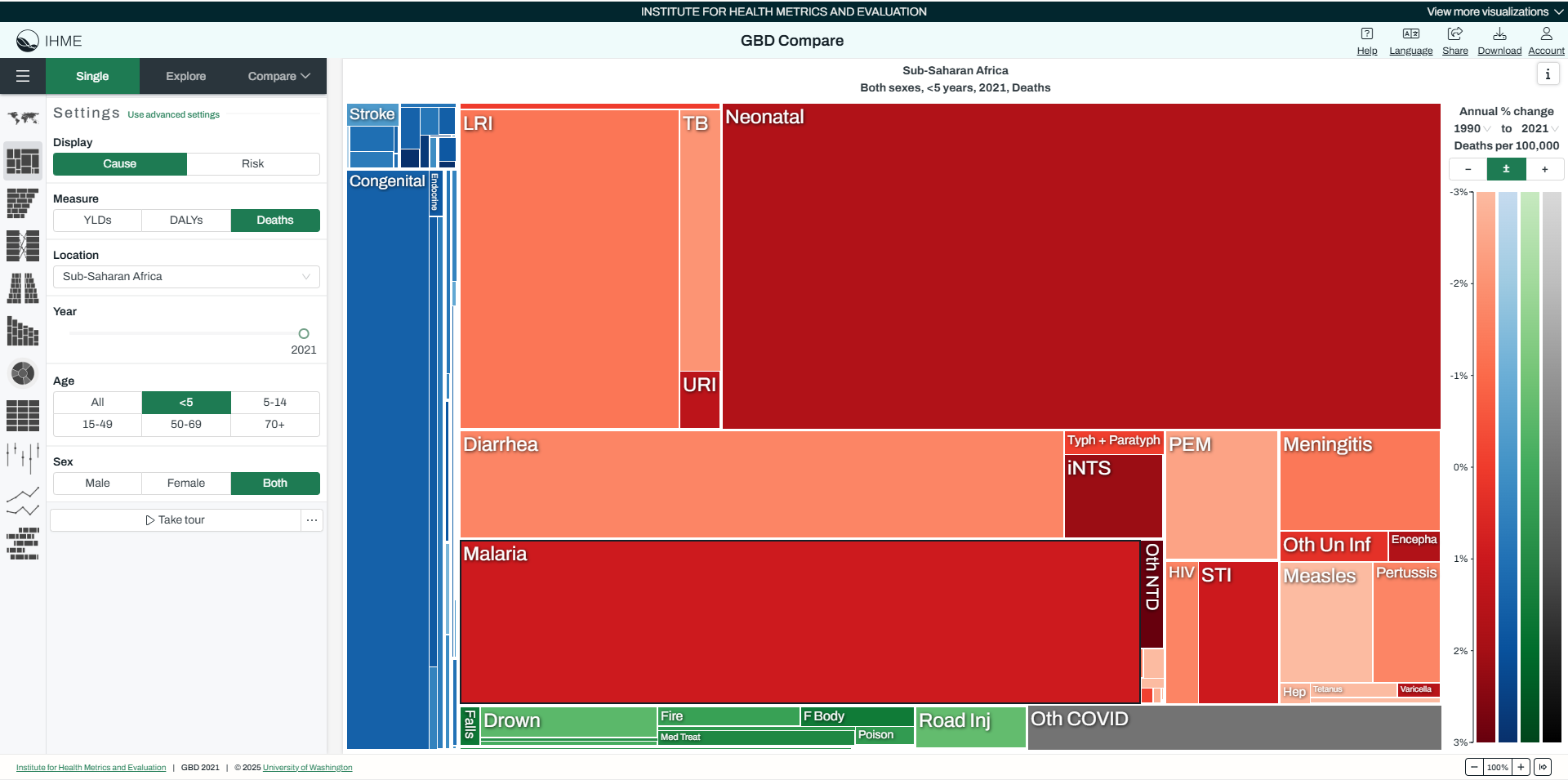
Malaria caused 15.8% of under-5 deaths in sub-Saharan Africa in 2021, according to estimates from the Institute for Health Metrics and Evaluation (IHME). IHME, GBD Compare Data Visualization, under-5 deaths in sub-Saharan Africa, 2021
- 4
"The manufacturer of RTS,S/AS01 recommends that the first dose of the vaccine is given to children aged from 5 months to 17 months. The first 3 doses should be administered at one-month intervals, with a fourth dose given 18 months after the third dose. The manufacturer of R21/Matrix-M recommends that the first dose of the vaccine is given to children aged from 5 months to 36 months of age. The first 3 doses should be administered at one-month intervals, with a fourth dose given 12 months after the third dose." WHO, Malaria vaccines: WHO position paper, 2024, p. 235
- 5
See cost per dose estimates in our CEA here. These estimates are sourced from Nature biotechnology, "Most effective malaria vaccine yet," 2023. As a point of comparison, standard EPI vaccines such as DTP, MPV or BCG all cost less than $1 per dose. See the UNICEF Product Menu for vaccines here.
- 6
“Vaccine efficacy against all clinical malaria episodes was 55.1% (95% CI, 50.5 to 59.3), and estimates were consistent across all case definitions and in both adjusted and intention- to-treat analyses.” RTS,S Clinical Trials Partnership 2011, p. 1868
- 7
“The target age group for malaria vaccine field efficacy trials has generally been children aged 5–17 months. When measuring the time to first malaria episode in this trial and dividing all the participants into two age groups of 5–17 months and 18–36 months, vaccine efficacy was significantly higher in the younger age group (78% [95% CI 73–82]) than in the older age group (70% [64–74]; p=0·024; appendix p 26). This finding was observed in both seasonal and standard sites: in the seasonal sites, vaccine efficacy in children aged 5–17 months was 79% (95% CI 73–84) and, at standard sites, this efficacy was 75% (65–83). There was also no evidence that vaccine efficacy was different in children aged 5–8 months compared with those aged 9–17 months.” Datoo et al 2024, p.539
- 8
"WHO updated their recommendation for malaria vaccines in October 2023. The updated recommendation is applicable to both RTS,S and R21 vaccines:
WHO recommends the programmatic use of malaria vaccines for the prevention of P. falciparum malaria in children living in malaria endemic areas, prioritizing areas of moderate and high transmission." WHO, "Malaria vaccines (RTS,S and R21)," 2024 - 9
PATH, Proposed support for malaria vaccine introduction acceleration (unpublished).
- 10
- Gavi’s implementation support amounts to $0.60 to $0.80 on introduction costs per child reached. See Gavi, Vaccine Funding Guidelines, April 2023, p. 8
- These costs are much less than the cost of introduction per child during the malaria vaccine implementation pilot program ($2.70 to $3.93 per child). PATH, Proposed support for malaria vaccine introduction acceleration, (unpublished).
- PATH and multiple other stakeholders have indicated Gavi's implementation support is insufficient. Source: Conversation with PATH, December 19 2023 (unpublished), other stakeholder conversations (unpublished).
- 11
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished). The RTS,S vaccine will be rolled out in Burkina Faso, and the four other countries will implement the R21 vaccine.
- 12
In review of a draft of this page, PATH told us that its activities will probably be split roughly evenly between subnational and national levels. PATH, comments on a draft of this page, December 16, 2024 (unpublished).
- 13
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 14
- PATH, Monitoring, Evaluation and Learning framework for GiveWell’s malaria vaccine introduction support, 2024 (unpublished).
- See Adjei 2023 for an example of a post-implementation evaluation from Ghana as part of the malaria vaccine pilot program.
- 15
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 16
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished),
Note: We learned in September 2024 that Uganda has opted to wait until April 2025 in order to roll out the vaccine nationally rather than incrementally (source: unpublished conversation with PATH, September 2024) - 17
Source: email from PATH, February 29, 2024 (unpublished).
- 18
The total budget for the activities is $18,205,272. We distributed $838,000 in the form of a bridge grant in January 2024 to allow the most time-sensitive activities to begin while PATH awaited a full funding decision. In March 2024, we recommended disbursing the remaining $17,367,272.
- 19
PATH, Malaria vaccine introduction support - proposed budget breakdown, 2024 (unpublished).
- 20
This benchmark is based on "moral weights," a system we use to quantify the benefits of different impacts (e.g. increased income vs reduced deaths). We benchmark to a value of 1, which we define as the value of doubling someone’s consumption for one year. Our estimate of the value of direct cash transfers is 0.00335 per dollar. For more on how we use moral weights, see this document.
- 21
"The cumulative supply availability of the two WHO-recommended and prequalified malaria vaccines is expected to meet the high demand, starting in 2024. Given the forecasted easing of supply constraints, the Framework for allocation of limited malaria vaccine supply will no longer be applied. As a result, Gavi has developed updated guidelines for countries to submit malaria vaccine scale-up plans. These updated guidelines will enable countries to expand the scope of malaria vaccine introduction beyond the areas initially approved by Gavi, in line with Gavi and WHO guidance." WHO, Malaria Policy Advisory Group Meeting: Update on malaria vaccines, March 2024, p. 1
- 22
For example, we model a 15 percentage point increase in syphilis treatment rates over 5 years as a result of Evidence Action's technical assistance in Liberia, a program we supported in 2020. We assume that PATH's support will lead to a smaller increase in malaria vaccine coverage.
- 23
GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished): “These inputs are needed in each country, but how this occurs will depend from country to country. Bottlenecks will also vary country to country
- For some countries certain enablers may be missing more than in others, which will lead to implementation delays.
- PATH’s approach is to identify and proactively address those bottlenecks. Don’t know ahead of time what specific bottlenecks will materialize, but will be in a position to learn about what those are. PATH has a lot of experience with vaccine rollouts, and knows what kinds of problems to look out for.”
- 24
For example: intervention mapping and targeting are typically the purview of NMCPs but delivery in this case will be the purview of immunization programs. Source: stakeholder conversations (unpublished)
- 25
"Public sector partners typically work independently (in silos) on either immunization or malaria. Institutional mechanisms to coordinate across programs are lacking or weak." PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 26
Source: stakeholder conversations (unpublished)
- 27
Source: stakeholder conversations (unpublished).
- 28
Source: stakeholder conversations (unpublished).
- 29
In Malawi during the MVIP, these committees comprised five members from each implementing region, who were trained in community messaging around the vaccine, along with EPI and NMCP staff. Source: in-person conversation with PATH, December 19, 2023 (unpublished)
- 30
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 31
PATH gave an example from the MVIP pilot in Ghana, where one region (Central Region) saw misinformation about the vaccine surge suddenly through social media and gain traction throughout the region. PATH had already developed a risk communication plan with the MoH which allowed them to act quickly. They put out targeted positive messaging about the vaccine, counteracting the rumors without directly addressing them, which they say worked to quell misinformation and vaccine hesitancy in this particular area. We heard about this same example separately from an outside expert we spoke to. Source: GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished), and stakeholder conversations (unpublished).
- 32
Source: stakeholder conversations (unpublished)
- 33
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 34
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 35
Source: GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished): "There are uncertainties PATH can control, some that are outside control. Won’t manage to avoid all roadblocks/shocks to implementation, but PATH support allows the trends to recover more quickly/easily than they would have otherwise.
- After health worker strikes, worked to emphasize catch-up which led to a spike in coverage.
- E.g. examples from MVIP including health worker strikes in Kenya (after which PATH helped drive forward a catch-up campaign), COVID-related vaccine stockouts in Ghana, and two tropical storms in Malawi, where vaccine coverage recovered relatively quickly after shock."
- 36
Source: stakeholder conversations (unpublished)
- 37
Source: stakeholder conversations (unpublished)
- 38
GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished): “MoHs are slow moving entities, burdened with a lot to do. Another PATH role is to drive national strategic goals. MoHs appreciate someone coming in and actualizing goals (e.g. getting a meeting to occur). PATH knows who needs to be there, and what needs to happen, which makes processes move faster. Because PATH is malaria vaccine-focused, it can counterbalance lack of focus from MoH (which has many different priorities) to ensure malaria vaccine planning work is moving forward.”
- 39
Source: stakeholder conversations (unpublished).
- 40
In our CEA, we model a 20% likelihood that we’re crowding out other actors' funding for these activities.
- 41
- Gavi is allocating implementation support funding in some countries through its vaccine introduction grants (VIGs), which amount to $0.60 to $0.80 per child, which is far less than estimated implementation costs from the MVIP pilot program ($2.70 to $3.93 per child based on costing studies). See PATH, Proposed support for malaria vaccine introduction acceleration (unpublished). PATH and other stakeholders have told us this funding is insufficient (source: Conversation with PATH, December 19, 2023 (unpublished), other stakeholder conversations (unpublished). Costs are expected to be somewhat lower per child during national rollouts than in a smaller-scale pilot, but the large difference in funding levels suggests that more funding for implementation support would be useful. We understand this as typical for Gavi, as its priority is on procuring and providing subsidized doses rather than providing full funding for robust implementation. Source: Conversation with PATH, December 19, 2023 (unpublished).
- "The Global Fund supports malaria interventions within the prevention and control toolbox, including vector control (insecticide treated nets (ITNs), indoor residual spraying (IRS)); chemoprevention (seasonal malaria chemoprevention, intermittent preventive treatment in pregnancy); case management (rapid diagnostic tests, artemisinin combination-based therapies, continuous quality improvement); and surveillance and programme management. The Global Fund does not currently finance procurement of malaria vaccines and ancillary equipment, as this is under Gavi’s mandate." Global Fund and Gavi, Malaria Vaccine: Guidelines on Gavi and Global Fund support for complementary interventions to facilitate the deployment of malaria vaccines, 2024
- President's Malaria Initiative (PMI)’s vaccine funding will likely be limited in the medium term due to its existing commitments to programs such as insecticide-treated nets and case management. PMI is contributing some funds to social behavioral change for malaria vaccines, but have indicated that they won’t be able to support TA or implementation costs at a large scale. (source: unpublished stakeholder conversations)
- 42
Target initial introduction dates, by country:
- DRC: July 2024
- Mozambique: July/Aug 2024
- Nigeria: Q4 2024
- Uganda: April 2025
- Burkina Faso: February 2024
Source: PATH, Approach to staged malaria vaccine introduction acceleration support, 2023, (unpublished).
Note: We learned in September 2024 that Uganda has opted to wait until April 2025 in order to roll out the vaccine nationally rather than incrementally (source: unpublished conversation with PATH, September 2024) - 43
Coverage of RTS,S-3 in the few years after introduction (pilot started in 2019):
- 73-81% between 2020-22 in Malawi
- 66-74% between 2020-22 in Ghana
- 60-72% between 2020-22 in Kenya
See PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 44
PATH’s role in other vaccine rollouts:
- “Polio: PATH worked on both the development and licensure of the vaccine; the Global Polio Eradication Initiative (GPEI) was responsible for implementation.
- Other vaccines: PATH played a central role in being the 'hub of the partnership wheel' (being in-country, coordinating partners)
- Along with WHO, PATH designed plans for vaccine rollout, then handed off to local in-country partners
- HPV vaccine: PATH led the demo projects, helped countries decide the best ways to rollout the vaccine. PATH supported 30 countries in doing this
- Rotavirus: PATH coordinated these interactions with WHO and CDC
- The Typhoid Vaccine Acceleration Consortium (TyVAC) Consortium: PATH, Oxford, Maryland, funded by GATES.”
Source: GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished)
- 45
Source: stakeholder conversations (unpublished)
- 46
Source: stakeholder conversations (unpublished)
- 47
This understanding is based on our conversations with stakeholders (unpublished)
- 48
We considered whether this factor might actually increase PATH’s marginal impact (e.g., strong government buy-in could make PATH’s TA better-received and thus more effective) rather than decrease it (e.g., there’s less work for PATH to do because governments are already committed to devoting resources to implementation). Because in this case there is strong buy-in and the program is highly likely to happen without the grant, we ultimately thought of this as a case against, rather than for, the grant.
- 49
Source: stakeholder conversations (unpublished)
- 50
We are aware of other TA partners in Burkina Faso, Nigeria, and DRC. We have not looked into whether there are also other partners in Mozambique and Uganda. Source: stakeholder conversations (unpublished).
- 51
Source: stakeholder conversations (unpublished)
- 52
Source: stakeholder conversations (unpublished)
- 53
Source: GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished)
- 54
Source: GiveWell's non-verbatim summary of a conversation with PATH, December 19, 2023 (unpublished)
- 55
- This is our impression based on PATH, Approach to staged malaria vaccine introduction acceleration support, 2023, (unpublished) and stakeholder conversations (unpublished).
- In review of a draft of this page, PATH told us that its activities will probably be split roughly evenly between subnational and national levels. PATH, comments on a draft of this page, December 16, 2024 (unpublished).
- 56
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished).
- 57
PATH's work will begin in early 2024, prior to vaccine introduction.
Target initial introduction dates, by country:- DRC: July 2024
- Mozambique: July/Aug 2024
- Nigeria: Q4 2024
- Uganda: October 2024
- Burkina Faso: February 2024
PATH, Approach to staged malaria vaccine introduction acceleration support, 2023 (unpublished)
- 58
Source: stakeholder conversations (unpublished)
- 59
Source: stakeholder conversations (unpublished)
- 60
Funding for these interventions comes largely from the Global Fund rather than from government budgets, and stakeholders noted that the Global Fund is strict about how its funding is used. While we heard concerns about this configuration at a broader level, in the medium term it appears that it stands as a bulwark against vaccines diverting resources for other malaria interventions within country budgets. Source: stakeholder conversations (unpublished).
- 61
Source: stakeholder conversations (unpublished)
- 62
Source: stakeholder conversations (unpublished)
- 63
Source: stakeholder conversations (unpublished)
- 64
Source: stakeholder conversations (unpublished)
- 65
We do adjust for the presence of SMC in our CEA, and malaria mortality estimates from IHME already contain corrections for the role of ITNs. However, we have not investigated this question more systematically.